More and more interesting news pops up each day about benefits of treating atrial fibrillation. Did anyone ever think treating your heart would also treat Alzheimer's disease? As it turns out, if your doctor treats your atrial fibrillation in a certain way, it could help prevent Alzheimer's and other related dementia diseases. Recent research has shown that someone with AF (when upper chambers cause blood to pool and increase potential of blood clots, stroke, heart failure and death) are almost twice as likely (44%) to develop Alzheimer's. This risk is especially relative to younger patients (less than 70 years of age) claims Dr. John D. Day, a heart rhythm specialist at the Heart Institute at Intermountain Medical Center in Salt Lake City, UT.
In the study, Day and his team compared the likelihood of those that received catheter ablations for their atrial fibrillation versus those that treated their AF with medications. Although the percentages are small in both, anything that could decrease one's likeliness to develop Alzheimer's would surely be accepted. And a small percentage of a very large population can make a big difference in a lot of people's lives. In the results, about 0.2% of patients that underwent catheter ablation developed Alzheimer's versus 0.9% that treated their AF with medications only. Approximately 0.4% treated with catheter ablation developed dementia compared to 1.9% if the AF was treated with medications.
In addition, the risk of dying (6% versus 23.5%), the risk of stroke (2.2% versus 4.7%), the risk of dementia and Alzheimer's diseases were all reduced in patients that received catheter ablation compared to those on medications.
Now, is this due to the side effects of medications or the catheter ablation procedure itself? Surely the catheter ablation wouldn't make AF go away completely and thee patients are on some kind of medication to keep it from occurring again?! Maybe the combination of the catheter and the medications made them less likely to develop Alzheimer's or dementia?
I do find it very interesting that there is a definite link of Alzheimer's with atrial fibrillation considering their extremely different modes of action. Alzheimer's affects the brain; atrial fibrillation, the heart. Alzheimer's is often due to a malformation in protein folding, reduced synthesis of the neurotransmitter acetylcholine or myelin breakdown in the brain; atrial fibrillation can be cause by hypertension, other primary heart diseases, lung diseases, excessive alcohol consumption, hyperthyroidism, etc. Alzheimer's gets progressively worse mentally; atrial fibrillation is not as aggressive or obvious. Alzheimer's is concerned with memory and thus, the cerebral cortex (front) of the brain; the heart is controlled by the medulla oblongata (back) of the brain. So what is the connection between the two main organs in the human body? Is it in the pons (the relay station linking the cerebral cortex and the medulla oblongata)? Is it a neurotransmitter common between the two, like acetylcholine? Is it a specific nerve, like the vagus nerve? Is it inherited? There are still multiple avenues to research, but hopefully with research like Dr. Day's, someone can find the vital link between atrial fibrillation and Alzheimer's soon and prevent thousands of cases of dementia.
Saturday, July 24, 2010
Wednesday, July 14, 2010
Atrial Fibrillation Quick Fix?!
Watch out folks...keep your eyes and ears open for a new atrial fibrillation procedure coming to town! Even though Europe has been doing this "new" technique for approximately 2 years now, Canada is in its trial stages and the United States have begun investigations into its future clinical usage.
Again, atrial fibrillation is the most common irregular heart rhythm worldwide. The upper chambers (atria) beat rapidly and spiradically, disturbing the heart's ability to pump blood efficiently to the lower chambers (venticles) and the rest of the body. AF is responsible for 20 percent of strokes...thus the importance of newer, more efficient procedures to assist more patients rapidly, effectively and also affordably!
Two doctors in a Toronto regional health center have treated at least six patients with this new ablation technology. For the traditional treatment, 4 catheters are placed in large veins in the neck and groin. For the new technology, only 1 catheter is placed (groin). The tissue destruction method targets and eliminates the part of the heart that causes the rhythm problems, just like other ablation techniques. So what makes this so special?
The procedure can be performed in 75 PERCENT LESS TIME! This means doctors can do more procedures per day, which means they can get to other patients faster and making everyone feel better quicker! Also, because it is done more efficiently, the patient does not have to be exposed to as much radiation! Yet another benefit for patients with this new procedure is the recovery time....a patient can be on their feet within 4 hours of the treatment rather than about a day. Why would a patient or a doctor not opt for this treatment?!
Again, atrial fibrillation is the most common irregular heart rhythm worldwide. The upper chambers (atria) beat rapidly and spiradically, disturbing the heart's ability to pump blood efficiently to the lower chambers (venticles) and the rest of the body. AF is responsible for 20 percent of strokes...thus the importance of newer, more efficient procedures to assist more patients rapidly, effectively and also affordably!
Two doctors in a Toronto regional health center have treated at least six patients with this new ablation technology. For the traditional treatment, 4 catheters are placed in large veins in the neck and groin. For the new technology, only 1 catheter is placed (groin). The tissue destruction method targets and eliminates the part of the heart that causes the rhythm problems, just like other ablation techniques. So what makes this so special?
The procedure can be performed in 75 PERCENT LESS TIME! This means doctors can do more procedures per day, which means they can get to other patients faster and making everyone feel better quicker! Also, because it is done more efficiently, the patient does not have to be exposed to as much radiation! Yet another benefit for patients with this new procedure is the recovery time....a patient can be on their feet within 4 hours of the treatment rather than about a day. Why would a patient or a doctor not opt for this treatment?!
Thursday, July 8, 2010
Arrhythmia Types in Children
As you may have noticed, there are various types of arrhythmias in adults. What about children? First I will list and then describe the multiple arrhythmias that children can have:
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
2. Tachycardia (Fast heart beat)
3. Supraventricular Tachycardia (SVT)
4. Wolff-Parkinson White Syndrome
5. Bradycardia (Slow heart beat)
6. Sick sinus syndrome
7. Complete Heart Block
Until you have a child that has an arrhythmia, you may not be particularly concerned about the differences between the types. But it is important to know their differences so that doctors can treat them appropriately and that you, as a parent, can be prepared for these treatments.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
Has your heart ever felt like it skipped a beat? No, not the I-feel-in-love skip a beat but an actual feeling like it randomly skipped a beat. What has actually happened is the heart beated too early (hence "premature"), causing the beat after the pause to be felt more forcefully. PAC occurs in the upper chamber (atria) and PVC occurs in the lower chamber (ventricles). These are considered arrhythmias but are not major concerns for the most part. There are no special treatments and there is really no specific cause. Your child may want to be seen by a cardiologist to make sure that the heart is ok. It is important to remember that this is VERY common in normal children and teenagers and it may even disappear!
2. Tachycardia (Fast heart beat)
Here, the definition of "fast" depends on the patient's age and physical activity. A normal resting heart rate for a newborn is normally considered tachycardic above 160 beats per minute. For teenagers, it is much lower at around 90 beats per minute that they are considered tachycardic. For any age, an exercising patient will have a lower resting heart rate than one that does not exercise on a regular basis. While exercising, a teenager may have a normal heart rate up to 200 beats per minute.
3. Supraventricular Tachycardia
By far, SVT is THE most common abnormal tachycardia in children. The fast heart rate involves both the upper and lower chambers (atria and ventricles) but is not life-threatenng for most people. Treatment is only considered if the episodes are long or frequent. The heart rate of an infant with an otherwise normal heart may reach up to 220 beats per minute...this may cause the infant to breathe faster than normal and be more lethargic. If this is the case, the situation must be diagnosed and treated to return the heart to a normal rate. Medication can prevent further episodes.
Oftentimes, the SVT is detected while the baby is still in the womb. If this is the case, the mother can take medications to slow the baby's heart rate. For older children, symptoms may include palpitations, dizziness, lightheadedness, chest pain, upset stomach or weakness. Oddly enough, a maneuver called a Valsalva maneuver can be taught to them to slow their own heart rate. This is a maneuver involving "straining", or closing the nose and mouth and trying to breathe out may be successful.
It is unusual for a child to be unable to enjoy normal activities. Older children may need more diagnostic tests and medications but will still have no restrictions on activities. The treatment for SVT involves stopping the current episode and preventing the next episode, which varies with the child's age. In an infant's case, taking them to the hospital may be the best option. For other children, putting ice on the face and/or gagging may be beneficial to stop a fast heart rhythm!
4. Wolff-Parkinson-White Syndrome (WPW)
Remember the electrical conduction pathway mentioned in the last blog? If an abnormal conduction pathway runs between the atria and ventricles, the signal may arrive at the ventricles sooner than normal. Named after the three people who first described it, WPW syndrome is recognized by certain changes on the EKG. Many patients with WPW do not have symptoms but are a risk for cardiac arrest. Often, but certainly not always, medication can help improve the condition but sometimes surgery or removing the irregular pathway via a catheter is necessary.

5. Bradycardia (Slow heart beat)
Again, what is too "slow" for a person depends on their age and physical activity. A newborn should not have less than an 80 beat per minute heart rate. On the other hand, a physically fit teenager may have a resting heart rate of 50 beats per minute.
6. Sick Sinus Syndrome
Ok, stretch all the way back to last week's blog and retrieve the information about the Sinus Node (SA node aka Pacemaker)....ok got it? Good...sometimes it doesn't work right and when it's work is severly disturbed, it is called sick sinus syndrome. The child may not have any regular symptoms of a cardiac patient but may be tired, dizzy or faint. Children with Sick Sinus Syndrome will have episodes of both too fast (tachy) or too slow (brady) heart rates. This is an unusual syndrome in children but a pacemaker would fix the problem in most cases, although medication may also be necessary.
7. Complete Heart Block
Heart block may be present at or even before birth (congenital) or may even be caused by a heart surgery. Heart blocks mean that the heart's electrical signal can't pass normally from the upper to the lower chambers. If the signal is blocked, the slower pacemaker sets in from the lower chambers of the heart. If this pace is not fast enough for the heart, an articial pacemaker is placed in the patient.
So have you realized the importance of the electrical conduction pathway of the heart yet?!? I hope this blog has helped you come to an understanding of the different arrhythmias that children can present. For the most part, careful observance and some TLC is just what they need.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
2. Tachycardia (Fast heart beat)
3. Supraventricular Tachycardia (SVT)
4. Wolff-Parkinson White Syndrome
5. Bradycardia (Slow heart beat)
6. Sick sinus syndrome
7. Complete Heart Block
Until you have a child that has an arrhythmia, you may not be particularly concerned about the differences between the types. But it is important to know their differences so that doctors can treat them appropriately and that you, as a parent, can be prepared for these treatments.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
Has your heart ever felt like it skipped a beat? No, not the I-feel-in-love skip a beat but an actual feeling like it randomly skipped a beat. What has actually happened is the heart beated too early (hence "premature"), causing the beat after the pause to be felt more forcefully. PAC occurs in the upper chamber (atria) and PVC occurs in the lower chamber (ventricles). These are considered arrhythmias but are not major concerns for the most part. There are no special treatments and there is really no specific cause. Your child may want to be seen by a cardiologist to make sure that the heart is ok. It is important to remember that this is VERY common in normal children and teenagers and it may even disappear!
2. Tachycardia (Fast heart beat)
Here, the definition of "fast" depends on the patient's age and physical activity. A normal resting heart rate for a newborn is normally considered tachycardic above 160 beats per minute. For teenagers, it is much lower at around 90 beats per minute that they are considered tachycardic. For any age, an exercising patient will have a lower resting heart rate than one that does not exercise on a regular basis. While exercising, a teenager may have a normal heart rate up to 200 beats per minute.
3. Supraventricular Tachycardia
By far, SVT is THE most common abnormal tachycardia in children. The fast heart rate involves both the upper and lower chambers (atria and ventricles) but is not life-threatenng for most people. Treatment is only considered if the episodes are long or frequent. The heart rate of an infant with an otherwise normal heart may reach up to 220 beats per minute...this may cause the infant to breathe faster than normal and be more lethargic. If this is the case, the situation must be diagnosed and treated to return the heart to a normal rate. Medication can prevent further episodes.
Oftentimes, the SVT is detected while the baby is still in the womb. If this is the case, the mother can take medications to slow the baby's heart rate. For older children, symptoms may include palpitations, dizziness, lightheadedness, chest pain, upset stomach or weakness. Oddly enough, a maneuver called a Valsalva maneuver can be taught to them to slow their own heart rate. This is a maneuver involving "straining", or closing the nose and mouth and trying to breathe out may be successful.
It is unusual for a child to be unable to enjoy normal activities. Older children may need more diagnostic tests and medications but will still have no restrictions on activities. The treatment for SVT involves stopping the current episode and preventing the next episode, which varies with the child's age. In an infant's case, taking them to the hospital may be the best option. For other children, putting ice on the face and/or gagging may be beneficial to stop a fast heart rhythm!
4. Wolff-Parkinson-White Syndrome (WPW)
Remember the electrical conduction pathway mentioned in the last blog? If an abnormal conduction pathway runs between the atria and ventricles, the signal may arrive at the ventricles sooner than normal. Named after the three people who first described it, WPW syndrome is recognized by certain changes on the EKG. Many patients with WPW do not have symptoms but are a risk for cardiac arrest. Often, but certainly not always, medication can help improve the condition but sometimes surgery or removing the irregular pathway via a catheter is necessary.

5. Bradycardia (Slow heart beat)
Again, what is too "slow" for a person depends on their age and physical activity. A newborn should not have less than an 80 beat per minute heart rate. On the other hand, a physically fit teenager may have a resting heart rate of 50 beats per minute.
6. Sick Sinus Syndrome
Ok, stretch all the way back to last week's blog and retrieve the information about the Sinus Node (SA node aka Pacemaker)....ok got it? Good...sometimes it doesn't work right and when it's work is severly disturbed, it is called sick sinus syndrome. The child may not have any regular symptoms of a cardiac patient but may be tired, dizzy or faint. Children with Sick Sinus Syndrome will have episodes of both too fast (tachy) or too slow (brady) heart rates. This is an unusual syndrome in children but a pacemaker would fix the problem in most cases, although medication may also be necessary.
7. Complete Heart Block
Heart block may be present at or even before birth (congenital) or may even be caused by a heart surgery. Heart blocks mean that the heart's electrical signal can't pass normally from the upper to the lower chambers. If the signal is blocked, the slower pacemaker sets in from the lower chambers of the heart. If this pace is not fast enough for the heart, an articial pacemaker is placed in the patient.
So have you realized the importance of the electrical conduction pathway of the heart yet?!? I hope this blog has helped you come to an understanding of the different arrhythmias that children can present. For the most part, careful observance and some TLC is just what they need.
Friday, July 2, 2010
EKG/ECG....what are these waves on an electrocardiogram?
As most people that have been in a hospital setting or have had any heart problems know, an EKG is the medical device that records the electrical activity of the heart. I have chosen to discuss the EKG in detail because in later blogs, there will be terms used concerning the waves found on a patient's EKG. Usually if a doctor hears a heart murmur, sees something he or she is curious about or the patient has been complaining of chest pain, the doctor will order an EKG. The EKG is capable of discovering arrhythmias, myocardial infarctions (heart attacks), atrial enlargement, ventricular hypertrophies, and bundle branch blocks.
Normally, there is a conduction pathway in which the electrical activity of the heart follows. Keep in mind that the action potentials in the cells (remember the sodium and potassium channels and depolarization/repolarization stuff?) that control muscle contraction follow the same pattern in the heart. Contractions in the heart are also caused by electrical action potentials. The normal conduction pathway in the heart is as follows:
1. Located at the top of the right atrium is the Sinoatrial Node (SA Node), which is commonly called the pacemaker of the heart. This is appropriate because this is the node that sets the rhythm of the heartbeat. While all of the heart's cells are capable of generating electrical impulses that trigger contraction, the SA nod controls the pace because it generates impulses slightly faster than the rest of the heart. The intrinsic rate of the Sinoatrial Node is about 60-100 beats per minute.
2. The Atrioventricular Node (AV Node) is conveniently located between the right atrium and the right ventricle within the atril septum. If the SA node fails to set the heart rhythm correctly, the AV node picks up the slack and is the secondary pacemaker. The AV node's normal intrinsic firing rate without stimulation from the SA node is 40-60 beats per minute.
3. The Bundle of His receives the stimulation from the AV node to the point of the apex of the fascicular branches, which lead to the Purkinje Fibers that innervate the ventricles. The intrinsic rate of the Bundle of His is between 40-60 beats per minute when there is no stimulation from the SA and AV node.
4. Located in the inner ventricular walls of the heart, the Purkinje fibers are the next step in the conduction pathway. During the ventricular contraction of the cardiac cycle, they carry the contraction impulse from the left and right bundle branch to the ventricles. Purkinje fibers are also capable of acting as the pacemaker but are not specifically designed for this purpose due to their generation of action potentials at lower frequencies than the SA or AV nodes. This serves as the last resort when the other pacemakers listed above fail.
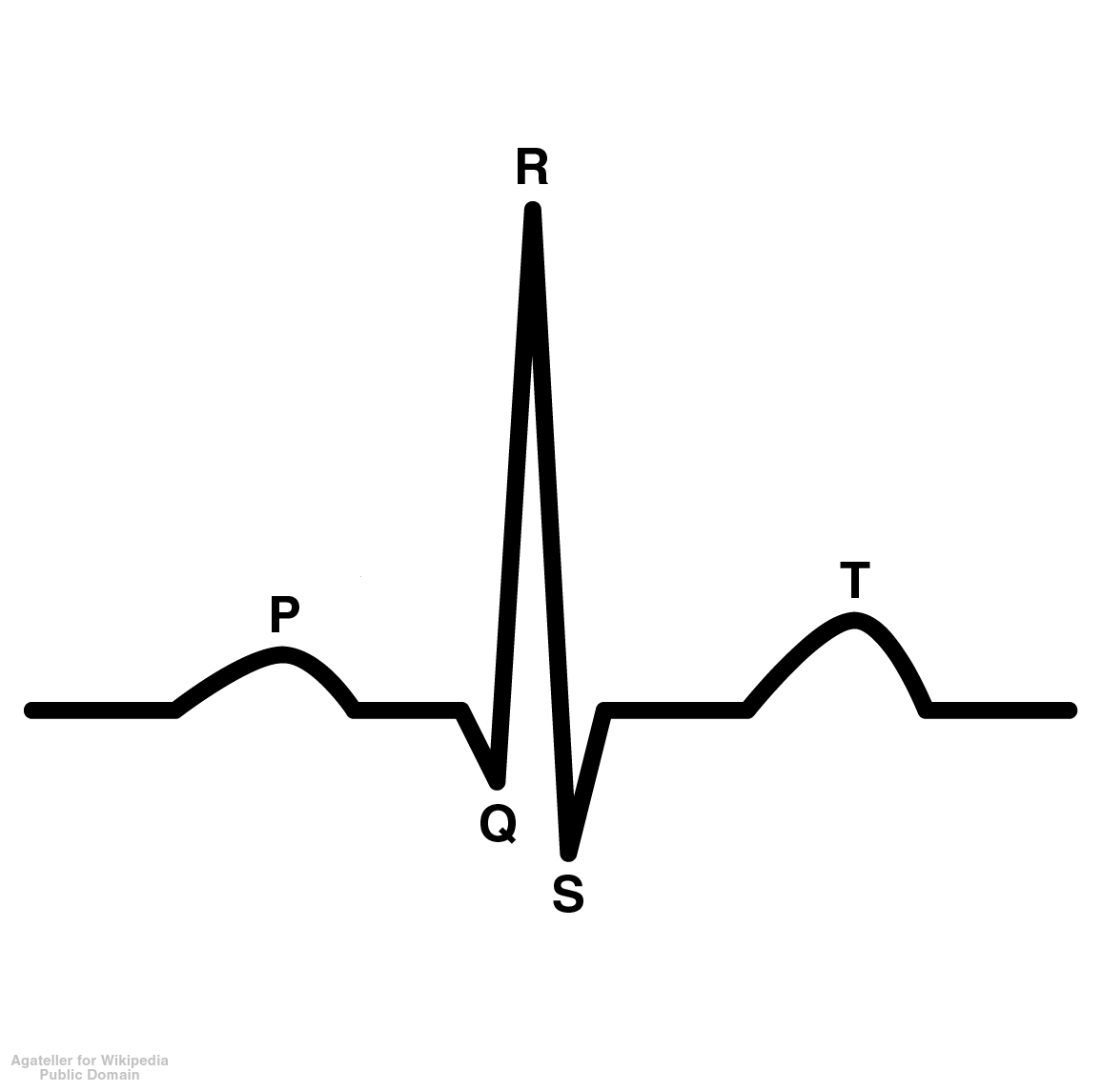
Now that we know the basics of the conduction pathway, let's talk about the actual EKG printout. Just what are all of those lines? Here is a picture of one with the different letters assigned to it:
P Wave=represents the depolarization of the atria (the beginning of the action potential when the cells become more positive, or less negative)
PR Interval=Represents the atria to ventricular conduction time (from the SA node to the AV node). This is measured from the onset of the P wave to the onset of the QRS complex and should last about 0.12-2.00 seconds.
QRS Complex=The QRS complex represents the depolarization of he right and left ventricles, which is coordinated by the Bundle of His and the Purkinje Fibers. A Q wave is a downward deflection after the P wave. An R wave is an upward reflection and the S wave is a downward deflection after the R wave. There may be multiple variations of this wave. The Q downstroke may not be present at all and the R upward deflection will show first or there may be an upward deflection after the S wave denoted R' which is representative of a bundle branch block. the duration, amplitude and morphology of the QRS complex is key to diagnosing cardiac arrhythmias, conduction abnormalities, ventricular hypertrophies, myocardial infarction or electrolyte derangements.
ST Segment=This serves as the isoelectric line from which to measure the amplitudes of the other waveforms. This is very important diagnostically for physicians because they can determine if the person has had a myocardial infarction (heart attack) by an elevation in this wave or ischemia, which is seen as a depression in the wave. ST elevation may indicate myocardial infarction (heart attack).
QT Interval=This represents the duration of activation and recovery of the ventricular muscle, which varies inversely with the heart rate. Thus the faster the heart rate, the shorter the QT interval. This QT interval does vary, the new QT Interval is called the corrected QT interval. This tends to be slightly longer for females and increases with age. A prolonged QT interval is a risk factor for ventricular tachyarrhythmias and sudden death.
T Wave=This represents ventricular repolarization. This is often times referred to as the refractory time for the heart, which is when the heart does not react to an action potential. The T-wave inversion (negative T waves the dip down instead of up) can be a sign of coronary ischemia, left ventricular hypertrophy or other disorders. There are other signs concerning the T wave that may lead to other diagnoses as well.
While one may still look at an EKG and not understand how to tell if one is normal or not, do not be alarmed! That's what the physician's job is! In basic terms, the EKG is printed out on boxes that have been scrutinizingly studied mathematically to determine what the normal height and width of certain waves should be. The height and width declares the amount of time in which a person is at a certain stage of their cardiac rhythm and this is how they make the correct diagnosis. But clearly this is one of the most powerful tools available to those that have heart problems and need a fast diagnosis.
Subscribe to:
Comments (Atom)
