You may have been wondering what are my options for treating arrhythmia that does not include all of these medications with side effects and costly procedures. Well I found a few natural treatments that may be of help, but please keep in mind they are not often enough to fully treat the arrhythmia. Please consult with your doctor about diagnosis and treatments. These things listed below may not be your complete solution but they will definitely not make it worse...it will certainly make you a healthier individual that leads a better lifestyle than one that could make your condition worse.
1. QUIT SMOKING
Clearly smoking is not good for your lungs or any other part of your respiratory system. So what would make you think it is good for your heart? Smoking can further complicate heart problems, so stopping as soon as possible is advisable. Even if you don't have a heart problem, please stop for your own health!
2. Avoid Alcohol
Alcohol can cause arrhythmias after one single drink simply because it depresses the central nervous system, keeping it from operating properly. (And no, drinking more than one will not make the arrhythmia go away nor will it make you feel better!) It is clearly never a smart move if you make the body stressed about anything you can avoid.
3. Relaxation
Have you ever taken a deep breath and suddenly felt your body relax just a little bit? Just the simple act of breathing deeply somehow puts the body at ease, right? Taking a deeper breath brings in more oxygen, which is delivered to the rest of the organs, calming the body. This helps combat stress and mental tensions as well, which will certainly make you feel better and is at least good for the sanity. (The bonus is that it is good for your health as well.)
4. Exercise!
By now, you probably feel like I'm a broken record that is just preaching away...But maybe you admit that any frustration/annoyance displaying on your face is because you know all of the above is true, right? Ok then, onward we go! Any excess weight is obviously weight that must be carried around every step of the way. This excess weight makes the heart have to work harder to get blood to all of the bigger (and no, not better) parts of the body. Now you don't have to look like a super model to be healthier than whatever your current state is. Not only can exercise help you lose weight, but it helps combat stress and releases endorphins in the body that are great for cardiac health. Surely any more sanity that can be gained from the daily stress of life would be warmly welcomed! Try simple exercises such as yoga, aerobics, fitness ball, cycling, dancing or walking on a daily basis to improve the overall health of your heart. I have found that having a partner (husband, wife, boyfriend, girlfriend, neighbor, parent, child, anyone!) in exercise keeps you entertained and motivated! You will have no idea how true this is until you have done a fitness class (or any exercise) with someone and then without someone. The difference is phenomenal-just make sure you don't spend more time talking than exercising!
5. Natural Herbs/Supplements
a. Omega-3 Fatty Acids
I know, these things are all over the news. What is so magical about something that has the word Fat and Acid in it? After extensive research into Omega-3 Fatty acids it has been determined that it strengthens the heart muscles and helps PREVENT arrhythmias!! Omega-3 Fatty Acid tablets can be found Over the Counter at most grocery stores and drug stores/pharmacy chains. It can also be found in foods (fish): such as sardines, salmon and mackerel. Consider adding these to your diet for a healthier heart!
b. Garlic
Whether you want to keep the vampires away or have a healthier heart, neither one hurts! Garlic has a ton of antioxidants (yes, the cool word that boosts your immunity--also found in blueberries and other yuumier tasting foods) and sulfur compounds that are great for overall heart health. Similar to Omega-3 Fatty Acids, garlic can be taken as a tablet or thrown in the mixture of your diet...but I'm pretty sure I know which one is less appealing. Don't forget to brush your teeth too...this won't help your heart but could be the deal breaker between getting a date with someone that makes your heart flutter or not. =)
c. Dilguard
Dilguard is a supplement that strengthens the heart muscles and provides immunity support as well. This herbal remedy is available as a vegetable capsule and should be taken on a regular basis in order to improve your cardiac health. Dilguard Plus capsules reduces platelet aggregation, lowers LDL (bad cholesterol) and maintain HDL (good cholesterol) levels.
6. QUIT STRESSING OUT
Quit stressing out about all of the things mentioned above that you may or may not be doing and just in general, quit stressing out as much as humanly possible. Stress alone may not be the cause of an arrhythmia but stress does lead to elevated blood pressure levels and cholesterol levels....which as we well know leads to heart problem later down the road. Stress triggers your "fight-or-flight" response, sending hormones flying and heart rates racing. The rate of blood flow increases, which increases blood pressure. Your body automatically releases fatty acids into the blood stream, which increases your cholesterol levels. Under chronic stress, the continued release of cortisol (hormone released from adrenal glands) seems to have some effect on where fat is deposited in the body, most often in the abdomen (again read #4 above-more weight=harder for the heart)! All of these things I just mentioned can lead to serious heart problems if the patient does not cut back on whatever it is that stresses them out! Remember those deep breaths I talked about earlier...they really help make you feel better, even if it's only temporary! We all know stress isn't going away any time soon and we also know it negatively affects our health...so really try to avoid it if at all possible. Whether it is financial, time-management, too much on your plate, loneliness, whatever...try to find someone or something that helps!
As mentioned above, none of these solutions are enough to make you completely, 100% healthy. If it were and we all followed all of these tips, we would not even need to have this discussion! Combining all of the above along with any additional treatments, medications or procedures that your doctor recommends will certainly improve your cardiac health. Don't try them all at once...this may overload you with more than you can handle. Maybe try adding one of these to the roster every week. Piling them all up at once may make you stressed out...which of course is not the goal!
If you have ever seen Bad Boys with Will Smith...Woosa...
Tuesday, August 24, 2010
Wednesday, August 18, 2010
Anticoagulants/Anti-Platelets as a Treatment for Patients with Heart Problems
Anticoagulant=blood thinner that makes it more difficult for the blood to clot (coagulate). They do not dissolve existing blood clots but prevent new clots from forming and from existing clots from getting larger.
Also known as blood thinners (although they really do not thin your blood), many patients with heart problems are prescribed anticoagulant medications. These are prescribed for people that are at increased risks for strokes because the most common stroke is caused by blood clots obstructing blood flow to the brain. For our purposes, anticoagulants are prescribed for others that are at increased risk for blood clots, such as those with an artificial heart valve or those with atrial fibrillation.
Three of the most commonly prescribed anticoagulants are Aspirin, Coumadin (generic: Warfarin Sodium) and Plavix. All of these drugs interfere with your body's natural ability to clot blood, which can be very dangerous in situations of large losses of blood (causes abnormal bleeding!). Therefore it is VERY important that these medications be taken exactly as prescribed!
Aspirin
Aspirin has an antiplatelet effect, which makes your blood platelets less likely to stick together and form clots. Aspirin is less likely to cause abnormal bleeding and is usually added in addition to a prescription anticoagulant.
Coumadin (Warfarin)
Warfarin is an anticoagulant that is more effective at preventing clot-caused strokes than Aspirin. Most people over age 60 with an atrial fibrillation will be prescribed a blood thinner. It has been shown that patients that have been taking Warfarin for a long period of time have reduced their chances of having a stroke by 70 percent or more! While the side effect of abnormal bleeding is a dangerous side effect, having a stroke is even more dangerous. It is important that it is taken exactly as prescribed. If a patient misses a dose, the patient should NOT take another one later to catch up. Always be sure to tell a new doctor, dentist, etc that you are taking Warfarin, especially when a new medication is being prescribed that may interfere or a procedure that causes bleeding.
Plavix
Anyone that has had one clot-related event (heart attack, stroke or heart-related chest pain) may be up to 9 times as likely to have another clot-related event. Plavix is the most researched (and one of, if not the most expensive) anti-platelet medicine. Many people take cholesterol and blood pressure medicines to help lower their risk of a heart attack or stroke. While reducing high blood pressure and cholesterol is extremely important, it’s also important to know that blood pressure and cholesterol medications do not directly address the formation of clots, which are the cause of most heart attacks and strokes. Therefore, blood pressure and cholesterol medications are NOT always ENOUGH to treat and prevent patients from having a clot-related event. Plavix addresses this important issue and is currently the #1 prescribed anti-platelet medication. The patient should not stop taking Plavix unless he or she consults their doctor first. Suddenly stopping Plavix can increase your risk of heart attack or stroke. People with stomach ulcers or conditions that cause bleeding should not use Plavix. Also patients that take any medication for heartburn or acid reflux (like Nexium or Prilosec) should not take Plavix.
While anticoagulants are not a direct treatment for arrhythmias, they are important in treating or preventing blood clots that may lead to a heart attack. Patients with atrial fibrillation are at increased risks for forming a blood clot in the upper chambers of their heart that can lead to a heart attack or stroke. Therefore, AF patients are commonly prescribed for anti-platelets. It is important to take these medications as prescribed because of the abnormal bleeding that can occur during surgeries or open wounds. But it is also important to remember that the abnormal bleeding is not as dangerous as the stroke or heart attack that can result from not taking these medications.
Also known as blood thinners (although they really do not thin your blood), many patients with heart problems are prescribed anticoagulant medications. These are prescribed for people that are at increased risks for strokes because the most common stroke is caused by blood clots obstructing blood flow to the brain. For our purposes, anticoagulants are prescribed for others that are at increased risk for blood clots, such as those with an artificial heart valve or those with atrial fibrillation.
Three of the most commonly prescribed anticoagulants are Aspirin, Coumadin (generic: Warfarin Sodium) and Plavix. All of these drugs interfere with your body's natural ability to clot blood, which can be very dangerous in situations of large losses of blood (causes abnormal bleeding!). Therefore it is VERY important that these medications be taken exactly as prescribed!
Aspirin
Aspirin has an antiplatelet effect, which makes your blood platelets less likely to stick together and form clots. Aspirin is less likely to cause abnormal bleeding and is usually added in addition to a prescription anticoagulant.
Coumadin (Warfarin)
Warfarin is an anticoagulant that is more effective at preventing clot-caused strokes than Aspirin. Most people over age 60 with an atrial fibrillation will be prescribed a blood thinner. It has been shown that patients that have been taking Warfarin for a long period of time have reduced their chances of having a stroke by 70 percent or more! While the side effect of abnormal bleeding is a dangerous side effect, having a stroke is even more dangerous. It is important that it is taken exactly as prescribed. If a patient misses a dose, the patient should NOT take another one later to catch up. Always be sure to tell a new doctor, dentist, etc that you are taking Warfarin, especially when a new medication is being prescribed that may interfere or a procedure that causes bleeding.
Plavix
Anyone that has had one clot-related event (heart attack, stroke or heart-related chest pain) may be up to 9 times as likely to have another clot-related event. Plavix is the most researched (and one of, if not the most expensive) anti-platelet medicine. Many people take cholesterol and blood pressure medicines to help lower their risk of a heart attack or stroke. While reducing high blood pressure and cholesterol is extremely important, it’s also important to know that blood pressure and cholesterol medications do not directly address the formation of clots, which are the cause of most heart attacks and strokes. Therefore, blood pressure and cholesterol medications are NOT always ENOUGH to treat and prevent patients from having a clot-related event. Plavix addresses this important issue and is currently the #1 prescribed anti-platelet medication. The patient should not stop taking Plavix unless he or she consults their doctor first. Suddenly stopping Plavix can increase your risk of heart attack or stroke. People with stomach ulcers or conditions that cause bleeding should not use Plavix. Also patients that take any medication for heartburn or acid reflux (like Nexium or Prilosec) should not take Plavix.
While anticoagulants are not a direct treatment for arrhythmias, they are important in treating or preventing blood clots that may lead to a heart attack. Patients with atrial fibrillation are at increased risks for forming a blood clot in the upper chambers of their heart that can lead to a heart attack or stroke. Therefore, AF patients are commonly prescribed for anti-platelets. It is important to take these medications as prescribed because of the abnormal bleeding that can occur during surgeries or open wounds. But it is also important to remember that the abnormal bleeding is not as dangerous as the stroke or heart attack that can result from not taking these medications.
Wednesday, August 11, 2010
Congenital Heart Defects & Diseases
Continuing along the same lines of the fetal circulation transforming into post-natal circulation brings us to the topic congenital heart defects. Congenital heart defect means it is a problem with the structure of the heart and is present at birth. It is the most common type of defect at birth. The problem with the structure arises from the fetal circulation not correctly transitioning to a normal post-natal circulation.
The majority of the structural defects arise from a valve not shutting completely or at all. There are a variety of defects that can occur:
1. Atrial Septal Defect (ASD) also known as Patent Foramen Ovale
Remember the foramen ovale that connects the right atria and the left atria...while inside the mother, this should remain open to shunt blood away from the lungs. But after birth, this valve should shut. If the valve does not shut, blood can move from the left atria (oxygenated blood) to the right atria (deoxygenated blood), which causes too much pressure to build up in the lungs or from the right atria to the left atria. With a large shunt (large hole between the atria), a person will be significantly short of breath because blood can reverse directions. A small shunt may not even be discovered until later in life and generally does not cause any major problems. By itself, an ASD could have no symptoms but patients are at an increased risk for atrial fibrillation, heart failure, pulmonary hypertension, and stroke. Treatment is usually not necessary if the defect is minor; if the defect is large, a simple procedure done via a catheter can fix it.
2. Ventral Septal Defect (VSD)
During pregnancy, a fetus' heart does not have two separate ventricles. As the fetus grows, a ventral wall between the right and left ventricle will form to separate them. However, if the wall does not completely form, a hole remains and is called a ventral septal defect. A baby may have no symptoms but can be seen by an EKG; it also may close by itself. If the defect is too large, too much blood will be pumped to the lungs (from the left ventricle to the right and then to the lungs) and can lead to heart failure. If the defect is large, symptoms may arise, such as: shortness of breath, fast or hard breathing, paleness and fast heart rate. VSD is one of the most common congenital heart defects and often occurs with other heart defects. Treatment is usually not necessary if the defect is minor; if the defect is large, a simple procedure done via a catheter can fix it.
3. Coarctation of the Aorta
Coarctation means narrowing...thus coarctation of the aorta means narrowing of the aorta! This makes it difficult for blood and nutrients to pass to the rest of the body. It can be seen with other congenital heart defects and is more common in those with genetic disorders. There may be no symptoms but there may be symptoms of shortness of breath, chest pain, poor growth, nosebleed and dizziness. Coarctation of the aorta can be cured with surgery and the patient may need to be prescribed blood pressure medications.
4. Patent Ductus Arteriosus
Remember the ductus arteriosus artery that connects the pulmonary artery to the aorta in a fetus to shunt blood away from the lungs? Patent means open...patent ductus arteriosus means the ductus arteriosus has not closed completely after birth. The condition leads to abnormal blood flow between the aorta and pulmonary artery, two major blood vessels that carry blood from the heart. PDA affects girls more than boys and is common in premature infants and those born with other congenital heart defects. The usual goal of treating PDA is to close the valve. The exception is when other heart defects are present and the PDA is keeping the patient alive. Medications, catheter procedure or surgery are among the options to repair the PDA.
5. Pulmonary Atresia
Atresia means closed or blocked. Pulmonary atresia occurs when the pulmonary valve (from the right ventricle to the lung) does not form properly; thus, blood cannot flow to the lungs to become oxygenated. Someone with pulmonary atresia may also have a weak tricuspid valve (valve between the right atria and right ventricle) and may occur with VSD. Prostaglandins are usually given to move blood into the lungs to become oxygenated by keeping the ductus arteriosus open. Other treatments include heart catheterization or open heart surgery.
As you may have noticed, most of the congenital heart defects occur from valves that are inappropriately opened or closed or even the wrong size. I will list some of the diseases that may be commonly heard of and what exactly they entail:
1. Cyanotic Heart Disease
This is a congenital heart defect that results in low blood oxygen levels. Any abnormal blood flow through the heart can cause the blood to not be oxygenated to the appropriate level. This can cause the child's skin to appear blue on the lips, fingers and toes! Medications are often administered or may need surgery to repair the defect causing the oxygen levels to be low.
2. Dextrocardia
Strangley enough, someone's heart can be tilted incorrectly! The heart is pointed toward the right side of the chest rather than the left. Most types of dextrocardia also occur with other abdomen or heart problems. In a rare case, the heart and other organs can mirror what they normally look like. In this case, no treatment is needed. In addition, the abdominal and chest organs in babies with dextrocardia may be abnormal and may not work correctly. If heart defects are present along with dextrocardia, surgery and medications may be necessary.
3. Hypoplastic Left Heart Syndrome
Hypoplastic Left Heart Syndrome occurs when the left heart (ventricle, mitral valve, aortic valve and aorta) do not develop completely. This is very rare and occurs in males more often than females. It causes the ventricle and aorta to be smaller than normal, which leads to the heart being unable to send enough blood to the rest of the body and overloads the right ventricle by forcing it to fulfill the duties of supplying the lungs and the rest of the body with blood. This eventually leads the right heart into heart failure. If it is known that the baby has hypoplastic heart syndrome before birth, medication will be given to keep the ductus arteriosus open in order for the baby to stay alive. If the ductus arteriosus is allowed to close, the patient could quickly die. The baby may seem normal when born but could have symptoms of blue skin, cold extremities, lethargy, poor pulse or rapid breathing. A ventilator may be necessary to help the baby breathe and will soon need surgeries to fix the hypoplastic left heart syndrome.
4. Transposition of the Great Vessels
A congenital heart defect in which the two major vessels that carry blood away from the heart (the aorta and pulmonary artery) are switched....a major problem. In transposition of the great vessels, the blood goes to the lungs, picks up oxygen, and then goes right back to the lungs without going to the body. Blood from the body returns to the heart and goes back to the body without ever picking up oxygen in the lungs. The patient will most likely be blue, feed poorly, be short of breath and have clubbing of the fingers or toes. The infant will immediately receive prostaglandins, which keep the ductus arteriosus open, allowing some mixing of the oxygenated and deoxygenated blood. A cardiac catheterization and a surgery called arterial switch procedure will be needed to permanently correct the problem. This must be done within the first week of the baby's life.
5. Tricuspid Atresia
The tricuspid heart valve is the valve between the right atria and ventricle. Atresia means blocked or closed. In tricuspid atresia, the tricuspid heart valve is missing or is not completely developed. While rare, 20% of the patients with this condition will have other heart problems. Blood ultimately cannot enter the lungs to pick up oxygen; thus, the infant's skin will be blue (cyanotic). Being extremely short of breath, the baby will need to be put on a ventilator to help it breathe and prostaglandin is used to maintain circulation of blood to the lungs. This condition always requires surgery within the first few days of life. Three surgeries may be necessary, two of which are called the Glenn shunt and Fontan procedure.
6. Tetralogy of Fallot
Tetra=4....4 related defects of the heart and its major blood vessels:
a. VSD (hole between left and right ventricle)
b. Narrowing of the pulmonary outflow tract (the valve and artery that connect the heart with the lungs)
c. Overriding aorta that is shifter over the right ventricle and VSD, instead of only coming out from the left ventricle
d. Thickened muscular wall of the right ventricle (hypertrophy=larger than normal)
Cyanosis (blue skin), difficulty feeding, failure to gain weight, passing out, clubbing of fingers, and poor development are all symptoms of tetralogy of fallot. Surgery is always required to correct the heart's 4 defects, and usually multiple surgeries. Most cases can be corrected with surgery and the patient can live an active, healthy life.
Clearly, medications and surgeries are the answers to correcting the majority of the congential heart defects. And even more obvious, the tranformation of the heart from fetal circulation to post-natal circulation is of utmost importance for a normal, heart-healthy baby.
The majority of the structural defects arise from a valve not shutting completely or at all. There are a variety of defects that can occur:
1. Atrial Septal Defect (ASD) also known as Patent Foramen Ovale
Remember the foramen ovale that connects the right atria and the left atria...while inside the mother, this should remain open to shunt blood away from the lungs. But after birth, this valve should shut. If the valve does not shut, blood can move from the left atria (oxygenated blood) to the right atria (deoxygenated blood), which causes too much pressure to build up in the lungs or from the right atria to the left atria. With a large shunt (large hole between the atria), a person will be significantly short of breath because blood can reverse directions. A small shunt may not even be discovered until later in life and generally does not cause any major problems. By itself, an ASD could have no symptoms but patients are at an increased risk for atrial fibrillation, heart failure, pulmonary hypertension, and stroke. Treatment is usually not necessary if the defect is minor; if the defect is large, a simple procedure done via a catheter can fix it.
2. Ventral Septal Defect (VSD)
During pregnancy, a fetus' heart does not have two separate ventricles. As the fetus grows, a ventral wall between the right and left ventricle will form to separate them. However, if the wall does not completely form, a hole remains and is called a ventral septal defect. A baby may have no symptoms but can be seen by an EKG; it also may close by itself. If the defect is too large, too much blood will be pumped to the lungs (from the left ventricle to the right and then to the lungs) and can lead to heart failure. If the defect is large, symptoms may arise, such as: shortness of breath, fast or hard breathing, paleness and fast heart rate. VSD is one of the most common congenital heart defects and often occurs with other heart defects. Treatment is usually not necessary if the defect is minor; if the defect is large, a simple procedure done via a catheter can fix it.
3. Coarctation of the Aorta
Coarctation means narrowing...thus coarctation of the aorta means narrowing of the aorta! This makes it difficult for blood and nutrients to pass to the rest of the body. It can be seen with other congenital heart defects and is more common in those with genetic disorders. There may be no symptoms but there may be symptoms of shortness of breath, chest pain, poor growth, nosebleed and dizziness. Coarctation of the aorta can be cured with surgery and the patient may need to be prescribed blood pressure medications.
4. Patent Ductus Arteriosus
Remember the ductus arteriosus artery that connects the pulmonary artery to the aorta in a fetus to shunt blood away from the lungs? Patent means open...patent ductus arteriosus means the ductus arteriosus has not closed completely after birth. The condition leads to abnormal blood flow between the aorta and pulmonary artery, two major blood vessels that carry blood from the heart. PDA affects girls more than boys and is common in premature infants and those born with other congenital heart defects. The usual goal of treating PDA is to close the valve. The exception is when other heart defects are present and the PDA is keeping the patient alive. Medications, catheter procedure or surgery are among the options to repair the PDA.
5. Pulmonary Atresia
Atresia means closed or blocked. Pulmonary atresia occurs when the pulmonary valve (from the right ventricle to the lung) does not form properly; thus, blood cannot flow to the lungs to become oxygenated. Someone with pulmonary atresia may also have a weak tricuspid valve (valve between the right atria and right ventricle) and may occur with VSD. Prostaglandins are usually given to move blood into the lungs to become oxygenated by keeping the ductus arteriosus open. Other treatments include heart catheterization or open heart surgery.
As you may have noticed, most of the congenital heart defects occur from valves that are inappropriately opened or closed or even the wrong size. I will list some of the diseases that may be commonly heard of and what exactly they entail:
1. Cyanotic Heart Disease
This is a congenital heart defect that results in low blood oxygen levels. Any abnormal blood flow through the heart can cause the blood to not be oxygenated to the appropriate level. This can cause the child's skin to appear blue on the lips, fingers and toes! Medications are often administered or may need surgery to repair the defect causing the oxygen levels to be low.
2. Dextrocardia
Strangley enough, someone's heart can be tilted incorrectly! The heart is pointed toward the right side of the chest rather than the left. Most types of dextrocardia also occur with other abdomen or heart problems. In a rare case, the heart and other organs can mirror what they normally look like. In this case, no treatment is needed. In addition, the abdominal and chest organs in babies with dextrocardia may be abnormal and may not work correctly. If heart defects are present along with dextrocardia, surgery and medications may be necessary.
3. Hypoplastic Left Heart Syndrome
Hypoplastic Left Heart Syndrome occurs when the left heart (ventricle, mitral valve, aortic valve and aorta) do not develop completely. This is very rare and occurs in males more often than females. It causes the ventricle and aorta to be smaller than normal, which leads to the heart being unable to send enough blood to the rest of the body and overloads the right ventricle by forcing it to fulfill the duties of supplying the lungs and the rest of the body with blood. This eventually leads the right heart into heart failure. If it is known that the baby has hypoplastic heart syndrome before birth, medication will be given to keep the ductus arteriosus open in order for the baby to stay alive. If the ductus arteriosus is allowed to close, the patient could quickly die. The baby may seem normal when born but could have symptoms of blue skin, cold extremities, lethargy, poor pulse or rapid breathing. A ventilator may be necessary to help the baby breathe and will soon need surgeries to fix the hypoplastic left heart syndrome.
4. Transposition of the Great Vessels
A congenital heart defect in which the two major vessels that carry blood away from the heart (the aorta and pulmonary artery) are switched....a major problem. In transposition of the great vessels, the blood goes to the lungs, picks up oxygen, and then goes right back to the lungs without going to the body. Blood from the body returns to the heart and goes back to the body without ever picking up oxygen in the lungs. The patient will most likely be blue, feed poorly, be short of breath and have clubbing of the fingers or toes. The infant will immediately receive prostaglandins, which keep the ductus arteriosus open, allowing some mixing of the oxygenated and deoxygenated blood. A cardiac catheterization and a surgery called arterial switch procedure will be needed to permanently correct the problem. This must be done within the first week of the baby's life.
5. Tricuspid Atresia
The tricuspid heart valve is the valve between the right atria and ventricle. Atresia means blocked or closed. In tricuspid atresia, the tricuspid heart valve is missing or is not completely developed. While rare, 20% of the patients with this condition will have other heart problems. Blood ultimately cannot enter the lungs to pick up oxygen; thus, the infant's skin will be blue (cyanotic). Being extremely short of breath, the baby will need to be put on a ventilator to help it breathe and prostaglandin is used to maintain circulation of blood to the lungs. This condition always requires surgery within the first few days of life. Three surgeries may be necessary, two of which are called the Glenn shunt and Fontan procedure.
6. Tetralogy of Fallot
Tetra=4....4 related defects of the heart and its major blood vessels:
a. VSD (hole between left and right ventricle)
b. Narrowing of the pulmonary outflow tract (the valve and artery that connect the heart with the lungs)
c. Overriding aorta that is shifter over the right ventricle and VSD, instead of only coming out from the left ventricle
d. Thickened muscular wall of the right ventricle (hypertrophy=larger than normal)
Cyanosis (blue skin), difficulty feeding, failure to gain weight, passing out, clubbing of fingers, and poor development are all symptoms of tetralogy of fallot. Surgery is always required to correct the heart's 4 defects, and usually multiple surgeries. Most cases can be corrected with surgery and the patient can live an active, healthy life.
Clearly, medications and surgeries are the answers to correcting the majority of the congential heart defects. And even more obvious, the tranformation of the heart from fetal circulation to post-natal circulation is of utmost importance for a normal, heart-healthy baby.
Friday, August 6, 2010
Fetal Circulation
Not everyone knows this but it's important in understanding infant arrhythmias and congenital heart defects: Fetal circulation is very different!! As a matter of fact, it seems as if everything is backwards. For now, I will discuss the circulation and later I will discuss the defects that can arise if fetal circulation does not make all of the proper changes to the normal postnatal circulation.
Normal Circulation/Flow of Blood Through the Heart
In a normal post-natal heart, blood flows in this order starting with deoxygenated blood:
Vena Cava (from the body and carries carbon dioxide)-->Right Atrium-->Triscuspid Valve-->Right Ventricle-->Pulmonary Arteries (carrying deoxygenated blood)-->Lungs-->Pulmonary Veins (carrying oxygenated blood)-->Left Atrium-->Mitral/Bicuspid Valve-->Left Ventricle-->Aorta (pumped to the rest of the body)
Below is a diagram of blood circulation in a normal heart: blue means deoxygenated blood and red is oxygenated blood.

Pressure in a normal post-natal heart is higher in the left heart (left atria and ventricle) than the right heart. The left heart is also larger, stronger and thicker than the right heart. This is due to the fact that the left heart must pump blood to the entire body and against gravity! The right heart simply has to pump blood into the lungs directly below it.
Fetal Circulation Similarities
1. The fetus has all of the same parts (2 atria, 2 ventricles, valves, arteries and veins) but as mentioned above may be different sizes.
2. The fetus receives deoxygenated blood into the right atrium.
Fetal Circulation Differences
1. The first and foremost important thing to recognize is that a fetus does not have mature lungs until approximately 36-37 weeks gestation. But the blood still needs to receive oxygen from somewhere...
2. Umbilical Vein
This is the somewhere that the oxygenated blood comes from. While veins typically carry deoxygenated blood from the body back to the heart to be oxygenated by the lungs, pulmonary veins and umbilical veins are different!! Again, fetal circulation is different! The UMBILICAL VEIN carries OXYGENATED blood from the mother's heart TO the PLACENTA.
3. Umbilical Arteries
Yes, plural. There are two arteries; as a matter of fact, when a baby is born this is one of the first things the doctor checks after cutting the umbilical cord. The doctor makes sure there are two arteries and one vein. Normally arteries carry oxygenated blood away from the heart to the body and pick up carbon dioxide to bring back to the lungs. BUT again, pulmonary arteries and umbilical arteries are different! The UMBILICAL ARTERIES bring DEOXYGENATED blood FROM the PLACENTA to the mother.
4. Foramen Ovale
Because the fetus does not have mature lungs to be able to exchange gases itself, blood that normally goes to the lungs must be shunted away from them in the fetus. The first of these shunts is the foramen ovale: this shunts blood from the right atrium to the left atrium (at the top of the heart) bypassing the right ventricle and the lungs. As opposed to the post-natal heart, the fetus' right heart has higher pressure than the left heart (DIFFERENT in yet another way)! This pressure differential pushes blood from the higher pressure heart to the lower pressure heart to avoid the lungs. The foramen ovale normally closes within 3 months of birth.
5. Ductus Arteriosus
The second cardiac shunt in the fetus is the ductus arteriosus. Any blood that has gotten to the right ventricle and not gone through the foramen ovale is shunted from the pulmonary arteries (normally carries deoxygenated blood to the lungs to become oxygenated) to the aorta (pumped to the rest of the body). Again, this bypasses the lungs. The ductus arteriosus typically closes once breathing regulates in the newborn baby.
6. Ductus Venosus
The ductus venosus is another shunt that is present in the fetus that is not present after birth. This does not directly involve blood flow in the heart but sends approximately 80% of the blood from the umbilical vein to the inferior vena cava (vein that carries blood from lower extremities back to the heart). The ductus venosus therefore bypasses the fetal liver. Within minutes of birth, the ductus venosus does not work but it will take 3-7 days for it to completely close.
As a general overview, everything above is basically how the fetal heart differs from that of a healthy, normal person after birth. As mentioned above, I will discuss how congenital heart defects and arrhythmias can be present at birth if something in the regular developmental cycle goes wrong.
Normal Circulation/Flow of Blood Through the Heart
In a normal post-natal heart, blood flows in this order starting with deoxygenated blood:
Vena Cava (from the body and carries carbon dioxide)-->Right Atrium-->Triscuspid Valve-->Right Ventricle-->Pulmonary Arteries (carrying deoxygenated blood)-->Lungs-->Pulmonary Veins (carrying oxygenated blood)-->Left Atrium-->Mitral/Bicuspid Valve-->Left Ventricle-->Aorta (pumped to the rest of the body)
Below is a diagram of blood circulation in a normal heart: blue means deoxygenated blood and red is oxygenated blood.

Pressure in a normal post-natal heart is higher in the left heart (left atria and ventricle) than the right heart. The left heart is also larger, stronger and thicker than the right heart. This is due to the fact that the left heart must pump blood to the entire body and against gravity! The right heart simply has to pump blood into the lungs directly below it.
Fetal Circulation Similarities
1. The fetus has all of the same parts (2 atria, 2 ventricles, valves, arteries and veins) but as mentioned above may be different sizes.
2. The fetus receives deoxygenated blood into the right atrium.
Fetal Circulation Differences
1. The first and foremost important thing to recognize is that a fetus does not have mature lungs until approximately 36-37 weeks gestation. But the blood still needs to receive oxygen from somewhere...
2. Umbilical Vein
This is the somewhere that the oxygenated blood comes from. While veins typically carry deoxygenated blood from the body back to the heart to be oxygenated by the lungs, pulmonary veins and umbilical veins are different!! Again, fetal circulation is different! The UMBILICAL VEIN carries OXYGENATED blood from the mother's heart TO the PLACENTA.
3. Umbilical Arteries
Yes, plural. There are two arteries; as a matter of fact, when a baby is born this is one of the first things the doctor checks after cutting the umbilical cord. The doctor makes sure there are two arteries and one vein. Normally arteries carry oxygenated blood away from the heart to the body and pick up carbon dioxide to bring back to the lungs. BUT again, pulmonary arteries and umbilical arteries are different! The UMBILICAL ARTERIES bring DEOXYGENATED blood FROM the PLACENTA to the mother.
4. Foramen Ovale
Because the fetus does not have mature lungs to be able to exchange gases itself, blood that normally goes to the lungs must be shunted away from them in the fetus. The first of these shunts is the foramen ovale: this shunts blood from the right atrium to the left atrium (at the top of the heart) bypassing the right ventricle and the lungs. As opposed to the post-natal heart, the fetus' right heart has higher pressure than the left heart (DIFFERENT in yet another way)! This pressure differential pushes blood from the higher pressure heart to the lower pressure heart to avoid the lungs. The foramen ovale normally closes within 3 months of birth.
5. Ductus Arteriosus
The second cardiac shunt in the fetus is the ductus arteriosus. Any blood that has gotten to the right ventricle and not gone through the foramen ovale is shunted from the pulmonary arteries (normally carries deoxygenated blood to the lungs to become oxygenated) to the aorta (pumped to the rest of the body). Again, this bypasses the lungs. The ductus arteriosus typically closes once breathing regulates in the newborn baby.
6. Ductus Venosus
The ductus venosus is another shunt that is present in the fetus that is not present after birth. This does not directly involve blood flow in the heart but sends approximately 80% of the blood from the umbilical vein to the inferior vena cava (vein that carries blood from lower extremities back to the heart). The ductus venosus therefore bypasses the fetal liver. Within minutes of birth, the ductus venosus does not work but it will take 3-7 days for it to completely close.
As a general overview, everything above is basically how the fetal heart differs from that of a healthy, normal person after birth. As mentioned above, I will discuss how congenital heart defects and arrhythmias can be present at birth if something in the regular developmental cycle goes wrong.
Saturday, July 24, 2010
Treating Heart Also Treats Mind...
More and more interesting news pops up each day about benefits of treating atrial fibrillation. Did anyone ever think treating your heart would also treat Alzheimer's disease? As it turns out, if your doctor treats your atrial fibrillation in a certain way, it could help prevent Alzheimer's and other related dementia diseases. Recent research has shown that someone with AF (when upper chambers cause blood to pool and increase potential of blood clots, stroke, heart failure and death) are almost twice as likely (44%) to develop Alzheimer's. This risk is especially relative to younger patients (less than 70 years of age) claims Dr. John D. Day, a heart rhythm specialist at the Heart Institute at Intermountain Medical Center in Salt Lake City, UT.
In the study, Day and his team compared the likelihood of those that received catheter ablations for their atrial fibrillation versus those that treated their AF with medications. Although the percentages are small in both, anything that could decrease one's likeliness to develop Alzheimer's would surely be accepted. And a small percentage of a very large population can make a big difference in a lot of people's lives. In the results, about 0.2% of patients that underwent catheter ablation developed Alzheimer's versus 0.9% that treated their AF with medications only. Approximately 0.4% treated with catheter ablation developed dementia compared to 1.9% if the AF was treated with medications.
In addition, the risk of dying (6% versus 23.5%), the risk of stroke (2.2% versus 4.7%), the risk of dementia and Alzheimer's diseases were all reduced in patients that received catheter ablation compared to those on medications.
Now, is this due to the side effects of medications or the catheter ablation procedure itself? Surely the catheter ablation wouldn't make AF go away completely and thee patients are on some kind of medication to keep it from occurring again?! Maybe the combination of the catheter and the medications made them less likely to develop Alzheimer's or dementia?
I do find it very interesting that there is a definite link of Alzheimer's with atrial fibrillation considering their extremely different modes of action. Alzheimer's affects the brain; atrial fibrillation, the heart. Alzheimer's is often due to a malformation in protein folding, reduced synthesis of the neurotransmitter acetylcholine or myelin breakdown in the brain; atrial fibrillation can be cause by hypertension, other primary heart diseases, lung diseases, excessive alcohol consumption, hyperthyroidism, etc. Alzheimer's gets progressively worse mentally; atrial fibrillation is not as aggressive or obvious. Alzheimer's is concerned with memory and thus, the cerebral cortex (front) of the brain; the heart is controlled by the medulla oblongata (back) of the brain. So what is the connection between the two main organs in the human body? Is it in the pons (the relay station linking the cerebral cortex and the medulla oblongata)? Is it a neurotransmitter common between the two, like acetylcholine? Is it a specific nerve, like the vagus nerve? Is it inherited? There are still multiple avenues to research, but hopefully with research like Dr. Day's, someone can find the vital link between atrial fibrillation and Alzheimer's soon and prevent thousands of cases of dementia.
In the study, Day and his team compared the likelihood of those that received catheter ablations for their atrial fibrillation versus those that treated their AF with medications. Although the percentages are small in both, anything that could decrease one's likeliness to develop Alzheimer's would surely be accepted. And a small percentage of a very large population can make a big difference in a lot of people's lives. In the results, about 0.2% of patients that underwent catheter ablation developed Alzheimer's versus 0.9% that treated their AF with medications only. Approximately 0.4% treated with catheter ablation developed dementia compared to 1.9% if the AF was treated with medications.
In addition, the risk of dying (6% versus 23.5%), the risk of stroke (2.2% versus 4.7%), the risk of dementia and Alzheimer's diseases were all reduced in patients that received catheter ablation compared to those on medications.
Now, is this due to the side effects of medications or the catheter ablation procedure itself? Surely the catheter ablation wouldn't make AF go away completely and thee patients are on some kind of medication to keep it from occurring again?! Maybe the combination of the catheter and the medications made them less likely to develop Alzheimer's or dementia?
I do find it very interesting that there is a definite link of Alzheimer's with atrial fibrillation considering their extremely different modes of action. Alzheimer's affects the brain; atrial fibrillation, the heart. Alzheimer's is often due to a malformation in protein folding, reduced synthesis of the neurotransmitter acetylcholine or myelin breakdown in the brain; atrial fibrillation can be cause by hypertension, other primary heart diseases, lung diseases, excessive alcohol consumption, hyperthyroidism, etc. Alzheimer's gets progressively worse mentally; atrial fibrillation is not as aggressive or obvious. Alzheimer's is concerned with memory and thus, the cerebral cortex (front) of the brain; the heart is controlled by the medulla oblongata (back) of the brain. So what is the connection between the two main organs in the human body? Is it in the pons (the relay station linking the cerebral cortex and the medulla oblongata)? Is it a neurotransmitter common between the two, like acetylcholine? Is it a specific nerve, like the vagus nerve? Is it inherited? There are still multiple avenues to research, but hopefully with research like Dr. Day's, someone can find the vital link between atrial fibrillation and Alzheimer's soon and prevent thousands of cases of dementia.
Wednesday, July 14, 2010
Atrial Fibrillation Quick Fix?!
Watch out folks...keep your eyes and ears open for a new atrial fibrillation procedure coming to town! Even though Europe has been doing this "new" technique for approximately 2 years now, Canada is in its trial stages and the United States have begun investigations into its future clinical usage.
Again, atrial fibrillation is the most common irregular heart rhythm worldwide. The upper chambers (atria) beat rapidly and spiradically, disturbing the heart's ability to pump blood efficiently to the lower chambers (venticles) and the rest of the body. AF is responsible for 20 percent of strokes...thus the importance of newer, more efficient procedures to assist more patients rapidly, effectively and also affordably!
Two doctors in a Toronto regional health center have treated at least six patients with this new ablation technology. For the traditional treatment, 4 catheters are placed in large veins in the neck and groin. For the new technology, only 1 catheter is placed (groin). The tissue destruction method targets and eliminates the part of the heart that causes the rhythm problems, just like other ablation techniques. So what makes this so special?
The procedure can be performed in 75 PERCENT LESS TIME! This means doctors can do more procedures per day, which means they can get to other patients faster and making everyone feel better quicker! Also, because it is done more efficiently, the patient does not have to be exposed to as much radiation! Yet another benefit for patients with this new procedure is the recovery time....a patient can be on their feet within 4 hours of the treatment rather than about a day. Why would a patient or a doctor not opt for this treatment?!
Again, atrial fibrillation is the most common irregular heart rhythm worldwide. The upper chambers (atria) beat rapidly and spiradically, disturbing the heart's ability to pump blood efficiently to the lower chambers (venticles) and the rest of the body. AF is responsible for 20 percent of strokes...thus the importance of newer, more efficient procedures to assist more patients rapidly, effectively and also affordably!
Two doctors in a Toronto regional health center have treated at least six patients with this new ablation technology. For the traditional treatment, 4 catheters are placed in large veins in the neck and groin. For the new technology, only 1 catheter is placed (groin). The tissue destruction method targets and eliminates the part of the heart that causes the rhythm problems, just like other ablation techniques. So what makes this so special?
The procedure can be performed in 75 PERCENT LESS TIME! This means doctors can do more procedures per day, which means they can get to other patients faster and making everyone feel better quicker! Also, because it is done more efficiently, the patient does not have to be exposed to as much radiation! Yet another benefit for patients with this new procedure is the recovery time....a patient can be on their feet within 4 hours of the treatment rather than about a day. Why would a patient or a doctor not opt for this treatment?!
Thursday, July 8, 2010
Arrhythmia Types in Children
As you may have noticed, there are various types of arrhythmias in adults. What about children? First I will list and then describe the multiple arrhythmias that children can have:
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
2. Tachycardia (Fast heart beat)
3. Supraventricular Tachycardia (SVT)
4. Wolff-Parkinson White Syndrome
5. Bradycardia (Slow heart beat)
6. Sick sinus syndrome
7. Complete Heart Block
Until you have a child that has an arrhythmia, you may not be particularly concerned about the differences between the types. But it is important to know their differences so that doctors can treat them appropriately and that you, as a parent, can be prepared for these treatments.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
Has your heart ever felt like it skipped a beat? No, not the I-feel-in-love skip a beat but an actual feeling like it randomly skipped a beat. What has actually happened is the heart beated too early (hence "premature"), causing the beat after the pause to be felt more forcefully. PAC occurs in the upper chamber (atria) and PVC occurs in the lower chamber (ventricles). These are considered arrhythmias but are not major concerns for the most part. There are no special treatments and there is really no specific cause. Your child may want to be seen by a cardiologist to make sure that the heart is ok. It is important to remember that this is VERY common in normal children and teenagers and it may even disappear!
2. Tachycardia (Fast heart beat)
Here, the definition of "fast" depends on the patient's age and physical activity. A normal resting heart rate for a newborn is normally considered tachycardic above 160 beats per minute. For teenagers, it is much lower at around 90 beats per minute that they are considered tachycardic. For any age, an exercising patient will have a lower resting heart rate than one that does not exercise on a regular basis. While exercising, a teenager may have a normal heart rate up to 200 beats per minute.
3. Supraventricular Tachycardia
By far, SVT is THE most common abnormal tachycardia in children. The fast heart rate involves both the upper and lower chambers (atria and ventricles) but is not life-threatenng for most people. Treatment is only considered if the episodes are long or frequent. The heart rate of an infant with an otherwise normal heart may reach up to 220 beats per minute...this may cause the infant to breathe faster than normal and be more lethargic. If this is the case, the situation must be diagnosed and treated to return the heart to a normal rate. Medication can prevent further episodes.
Oftentimes, the SVT is detected while the baby is still in the womb. If this is the case, the mother can take medications to slow the baby's heart rate. For older children, symptoms may include palpitations, dizziness, lightheadedness, chest pain, upset stomach or weakness. Oddly enough, a maneuver called a Valsalva maneuver can be taught to them to slow their own heart rate. This is a maneuver involving "straining", or closing the nose and mouth and trying to breathe out may be successful.
It is unusual for a child to be unable to enjoy normal activities. Older children may need more diagnostic tests and medications but will still have no restrictions on activities. The treatment for SVT involves stopping the current episode and preventing the next episode, which varies with the child's age. In an infant's case, taking them to the hospital may be the best option. For other children, putting ice on the face and/or gagging may be beneficial to stop a fast heart rhythm!
4. Wolff-Parkinson-White Syndrome (WPW)
Remember the electrical conduction pathway mentioned in the last blog? If an abnormal conduction pathway runs between the atria and ventricles, the signal may arrive at the ventricles sooner than normal. Named after the three people who first described it, WPW syndrome is recognized by certain changes on the EKG. Many patients with WPW do not have symptoms but are a risk for cardiac arrest. Often, but certainly not always, medication can help improve the condition but sometimes surgery or removing the irregular pathway via a catheter is necessary.

5. Bradycardia (Slow heart beat)
Again, what is too "slow" for a person depends on their age and physical activity. A newborn should not have less than an 80 beat per minute heart rate. On the other hand, a physically fit teenager may have a resting heart rate of 50 beats per minute.
6. Sick Sinus Syndrome
Ok, stretch all the way back to last week's blog and retrieve the information about the Sinus Node (SA node aka Pacemaker)....ok got it? Good...sometimes it doesn't work right and when it's work is severly disturbed, it is called sick sinus syndrome. The child may not have any regular symptoms of a cardiac patient but may be tired, dizzy or faint. Children with Sick Sinus Syndrome will have episodes of both too fast (tachy) or too slow (brady) heart rates. This is an unusual syndrome in children but a pacemaker would fix the problem in most cases, although medication may also be necessary.
7. Complete Heart Block
Heart block may be present at or even before birth (congenital) or may even be caused by a heart surgery. Heart blocks mean that the heart's electrical signal can't pass normally from the upper to the lower chambers. If the signal is blocked, the slower pacemaker sets in from the lower chambers of the heart. If this pace is not fast enough for the heart, an articial pacemaker is placed in the patient.
So have you realized the importance of the electrical conduction pathway of the heart yet?!? I hope this blog has helped you come to an understanding of the different arrhythmias that children can present. For the most part, careful observance and some TLC is just what they need.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
2. Tachycardia (Fast heart beat)
3. Supraventricular Tachycardia (SVT)
4. Wolff-Parkinson White Syndrome
5. Bradycardia (Slow heart beat)
6. Sick sinus syndrome
7. Complete Heart Block
Until you have a child that has an arrhythmia, you may not be particularly concerned about the differences between the types. But it is important to know their differences so that doctors can treat them appropriately and that you, as a parent, can be prepared for these treatments.
1. Premature Atrial Contraction (PAC) and Premature Ventricular Contraction (PVC)
Has your heart ever felt like it skipped a beat? No, not the I-feel-in-love skip a beat but an actual feeling like it randomly skipped a beat. What has actually happened is the heart beated too early (hence "premature"), causing the beat after the pause to be felt more forcefully. PAC occurs in the upper chamber (atria) and PVC occurs in the lower chamber (ventricles). These are considered arrhythmias but are not major concerns for the most part. There are no special treatments and there is really no specific cause. Your child may want to be seen by a cardiologist to make sure that the heart is ok. It is important to remember that this is VERY common in normal children and teenagers and it may even disappear!
2. Tachycardia (Fast heart beat)
Here, the definition of "fast" depends on the patient's age and physical activity. A normal resting heart rate for a newborn is normally considered tachycardic above 160 beats per minute. For teenagers, it is much lower at around 90 beats per minute that they are considered tachycardic. For any age, an exercising patient will have a lower resting heart rate than one that does not exercise on a regular basis. While exercising, a teenager may have a normal heart rate up to 200 beats per minute.
3. Supraventricular Tachycardia
By far, SVT is THE most common abnormal tachycardia in children. The fast heart rate involves both the upper and lower chambers (atria and ventricles) but is not life-threatenng for most people. Treatment is only considered if the episodes are long or frequent. The heart rate of an infant with an otherwise normal heart may reach up to 220 beats per minute...this may cause the infant to breathe faster than normal and be more lethargic. If this is the case, the situation must be diagnosed and treated to return the heart to a normal rate. Medication can prevent further episodes.
Oftentimes, the SVT is detected while the baby is still in the womb. If this is the case, the mother can take medications to slow the baby's heart rate. For older children, symptoms may include palpitations, dizziness, lightheadedness, chest pain, upset stomach or weakness. Oddly enough, a maneuver called a Valsalva maneuver can be taught to them to slow their own heart rate. This is a maneuver involving "straining", or closing the nose and mouth and trying to breathe out may be successful.
It is unusual for a child to be unable to enjoy normal activities. Older children may need more diagnostic tests and medications but will still have no restrictions on activities. The treatment for SVT involves stopping the current episode and preventing the next episode, which varies with the child's age. In an infant's case, taking them to the hospital may be the best option. For other children, putting ice on the face and/or gagging may be beneficial to stop a fast heart rhythm!
4. Wolff-Parkinson-White Syndrome (WPW)
Remember the electrical conduction pathway mentioned in the last blog? If an abnormal conduction pathway runs between the atria and ventricles, the signal may arrive at the ventricles sooner than normal. Named after the three people who first described it, WPW syndrome is recognized by certain changes on the EKG. Many patients with WPW do not have symptoms but are a risk for cardiac arrest. Often, but certainly not always, medication can help improve the condition but sometimes surgery or removing the irregular pathway via a catheter is necessary.

5. Bradycardia (Slow heart beat)
Again, what is too "slow" for a person depends on their age and physical activity. A newborn should not have less than an 80 beat per minute heart rate. On the other hand, a physically fit teenager may have a resting heart rate of 50 beats per minute.
6. Sick Sinus Syndrome
Ok, stretch all the way back to last week's blog and retrieve the information about the Sinus Node (SA node aka Pacemaker)....ok got it? Good...sometimes it doesn't work right and when it's work is severly disturbed, it is called sick sinus syndrome. The child may not have any regular symptoms of a cardiac patient but may be tired, dizzy or faint. Children with Sick Sinus Syndrome will have episodes of both too fast (tachy) or too slow (brady) heart rates. This is an unusual syndrome in children but a pacemaker would fix the problem in most cases, although medication may also be necessary.
7. Complete Heart Block
Heart block may be present at or even before birth (congenital) or may even be caused by a heart surgery. Heart blocks mean that the heart's electrical signal can't pass normally from the upper to the lower chambers. If the signal is blocked, the slower pacemaker sets in from the lower chambers of the heart. If this pace is not fast enough for the heart, an articial pacemaker is placed in the patient.
So have you realized the importance of the electrical conduction pathway of the heart yet?!? I hope this blog has helped you come to an understanding of the different arrhythmias that children can present. For the most part, careful observance and some TLC is just what they need.
Friday, July 2, 2010
EKG/ECG....what are these waves on an electrocardiogram?
As most people that have been in a hospital setting or have had any heart problems know, an EKG is the medical device that records the electrical activity of the heart. I have chosen to discuss the EKG in detail because in later blogs, there will be terms used concerning the waves found on a patient's EKG. Usually if a doctor hears a heart murmur, sees something he or she is curious about or the patient has been complaining of chest pain, the doctor will order an EKG. The EKG is capable of discovering arrhythmias, myocardial infarctions (heart attacks), atrial enlargement, ventricular hypertrophies, and bundle branch blocks.
Normally, there is a conduction pathway in which the electrical activity of the heart follows. Keep in mind that the action potentials in the cells (remember the sodium and potassium channels and depolarization/repolarization stuff?) that control muscle contraction follow the same pattern in the heart. Contractions in the heart are also caused by electrical action potentials. The normal conduction pathway in the heart is as follows:
1. Located at the top of the right atrium is the Sinoatrial Node (SA Node), which is commonly called the pacemaker of the heart. This is appropriate because this is the node that sets the rhythm of the heartbeat. While all of the heart's cells are capable of generating electrical impulses that trigger contraction, the SA nod controls the pace because it generates impulses slightly faster than the rest of the heart. The intrinsic rate of the Sinoatrial Node is about 60-100 beats per minute.
2. The Atrioventricular Node (AV Node) is conveniently located between the right atrium and the right ventricle within the atril septum. If the SA node fails to set the heart rhythm correctly, the AV node picks up the slack and is the secondary pacemaker. The AV node's normal intrinsic firing rate without stimulation from the SA node is 40-60 beats per minute.
3. The Bundle of His receives the stimulation from the AV node to the point of the apex of the fascicular branches, which lead to the Purkinje Fibers that innervate the ventricles. The intrinsic rate of the Bundle of His is between 40-60 beats per minute when there is no stimulation from the SA and AV node.
4. Located in the inner ventricular walls of the heart, the Purkinje fibers are the next step in the conduction pathway. During the ventricular contraction of the cardiac cycle, they carry the contraction impulse from the left and right bundle branch to the ventricles. Purkinje fibers are also capable of acting as the pacemaker but are not specifically designed for this purpose due to their generation of action potentials at lower frequencies than the SA or AV nodes. This serves as the last resort when the other pacemakers listed above fail.
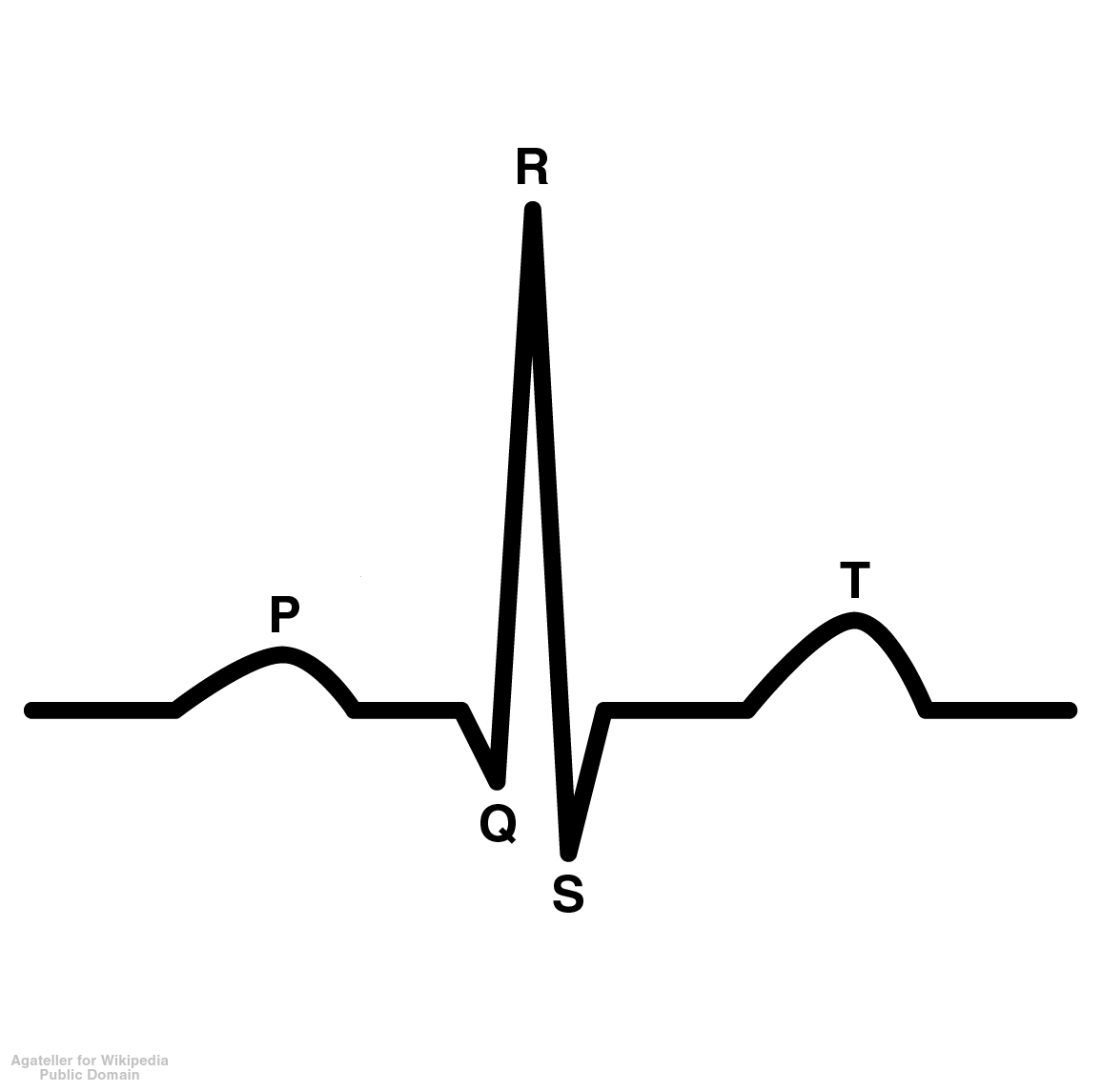
Now that we know the basics of the conduction pathway, let's talk about the actual EKG printout. Just what are all of those lines? Here is a picture of one with the different letters assigned to it:
P Wave=represents the depolarization of the atria (the beginning of the action potential when the cells become more positive, or less negative)
PR Interval=Represents the atria to ventricular conduction time (from the SA node to the AV node). This is measured from the onset of the P wave to the onset of the QRS complex and should last about 0.12-2.00 seconds.
QRS Complex=The QRS complex represents the depolarization of he right and left ventricles, which is coordinated by the Bundle of His and the Purkinje Fibers. A Q wave is a downward deflection after the P wave. An R wave is an upward reflection and the S wave is a downward deflection after the R wave. There may be multiple variations of this wave. The Q downstroke may not be present at all and the R upward deflection will show first or there may be an upward deflection after the S wave denoted R' which is representative of a bundle branch block. the duration, amplitude and morphology of the QRS complex is key to diagnosing cardiac arrhythmias, conduction abnormalities, ventricular hypertrophies, myocardial infarction or electrolyte derangements.
ST Segment=This serves as the isoelectric line from which to measure the amplitudes of the other waveforms. This is very important diagnostically for physicians because they can determine if the person has had a myocardial infarction (heart attack) by an elevation in this wave or ischemia, which is seen as a depression in the wave. ST elevation may indicate myocardial infarction (heart attack).
QT Interval=This represents the duration of activation and recovery of the ventricular muscle, which varies inversely with the heart rate. Thus the faster the heart rate, the shorter the QT interval. This QT interval does vary, the new QT Interval is called the corrected QT interval. This tends to be slightly longer for females and increases with age. A prolonged QT interval is a risk factor for ventricular tachyarrhythmias and sudden death.
T Wave=This represents ventricular repolarization. This is often times referred to as the refractory time for the heart, which is when the heart does not react to an action potential. The T-wave inversion (negative T waves the dip down instead of up) can be a sign of coronary ischemia, left ventricular hypertrophy or other disorders. There are other signs concerning the T wave that may lead to other diagnoses as well.
While one may still look at an EKG and not understand how to tell if one is normal or not, do not be alarmed! That's what the physician's job is! In basic terms, the EKG is printed out on boxes that have been scrutinizingly studied mathematically to determine what the normal height and width of certain waves should be. The height and width declares the amount of time in which a person is at a certain stage of their cardiac rhythm and this is how they make the correct diagnosis. But clearly this is one of the most powerful tools available to those that have heart problems and need a fast diagnosis.
Wednesday, June 23, 2010
Is coffee the miracle drug?
Coffee and Arrhythmias
For all you coffee drinkers out there that are concerned it is costing your heart some trouble...have no fear for a new large survey is here.
Brought on by the common concern that caffeine can make one's "heart flutter" researchers at Kaiser Permanente in Oakland, California decided to look into the amount of hospitalizations that java drinkers have versus those that avoid it altogether. They have found that coffee is not a determining factor for heart hospitalizations....so keep chugging away.
Not only does coffee not send you to the hospital clutching your chest but evidence from this research show that it may keep you from making that trip! The study began in the 1970s and 1980s with 130,000 men and women ranging in age from 18 to 90 years old. Compared with those that avoid coffee altogether, of those drinking 4+ cups per day were 18% less likely to be hospitalized for heart arrhythmia. Those drinking 1-3 cups were only 7% less likely to be hospitalized.
You may be wondering about the other lifestyle choices these 130,000 people made such as smoking. The researchers found that even when smoking status, gender, weight, cardiac history and education differences were all taken into account, the 4+ cups of coffee a day still kept them from a trip to the hospital for their heart. One blogger disagrees with the results: "I do not blame coffee intake FOR the arrhythmia but I do blame it for drastically making it worse. Last year, I gave up coffee for Lent. After three weeks, the arrhythmia was almost gone." So is this one person that blogged about this the exception or are there others like him?
Coffee and Strokes
Not long after the discovery was released about coffee not linked to arrhythmias it was determined that coffee was also associated with lower stroke risk! The study began in the mid 1990s with health records of more than 20,000 European men and women between 39 and 79 years old. The research was done at the University of Cambridge in England with people that were free of stroke history, heart disease and cancer in the mid 1990s. There were 855 strokes in these 120,000 people over the next 12 years. As it turns out though, coffee drinkers (drip grind, decaffeinated or even lowly instant) were only 71 percent as likely to have had a stroke as those that avoided the java. Smoking, physical activity, weight, tea drinking, blood pressure and cholesterol were all taken into account in this research.
This research did not seem to be dose-dependent: those that drank one cup of coffee a day or four had the same percentage of fewer strokes. Even with these results, the mechanism of action is unknown. There have even been some studies showing that because of the high antioxidant amounts in coffee, it improves insulin sensitivity and glucose metabolism. Thus, it is beneficial for those with diabetes by improving the body's response to insulin! Why is drinking coffee associated with lower stroke risk, less hospitalizations due to arrhythmias and better insulin sensitivity? Is it truly a miracle drug after all?
The coffee and arrhythmia link: http://www.sciencenews.org/view/generic/id/56862/title/Coffee_not_linked_to_heart_arrhythmia
The coffee and stroke link: http://www.sciencenews.org/view/generic/id/56701/title/Coffee_associated_with_lower_stroke_risk
For all you coffee drinkers out there that are concerned it is costing your heart some trouble...have no fear for a new large survey is here.
Brought on by the common concern that caffeine can make one's "heart flutter" researchers at Kaiser Permanente in Oakland, California decided to look into the amount of hospitalizations that java drinkers have versus those that avoid it altogether. They have found that coffee is not a determining factor for heart hospitalizations....so keep chugging away.
Not only does coffee not send you to the hospital clutching your chest but evidence from this research show that it may keep you from making that trip! The study began in the 1970s and 1980s with 130,000 men and women ranging in age from 18 to 90 years old. Compared with those that avoid coffee altogether, of those drinking 4+ cups per day were 18% less likely to be hospitalized for heart arrhythmia. Those drinking 1-3 cups were only 7% less likely to be hospitalized.
You may be wondering about the other lifestyle choices these 130,000 people made such as smoking. The researchers found that even when smoking status, gender, weight, cardiac history and education differences were all taken into account, the 4+ cups of coffee a day still kept them from a trip to the hospital for their heart. One blogger disagrees with the results: "I do not blame coffee intake FOR the arrhythmia but I do blame it for drastically making it worse. Last year, I gave up coffee for Lent. After three weeks, the arrhythmia was almost gone." So is this one person that blogged about this the exception or are there others like him?
Coffee and Strokes
Not long after the discovery was released about coffee not linked to arrhythmias it was determined that coffee was also associated with lower stroke risk! The study began in the mid 1990s with health records of more than 20,000 European men and women between 39 and 79 years old. The research was done at the University of Cambridge in England with people that were free of stroke history, heart disease and cancer in the mid 1990s. There were 855 strokes in these 120,000 people over the next 12 years. As it turns out though, coffee drinkers (drip grind, decaffeinated or even lowly instant) were only 71 percent as likely to have had a stroke as those that avoided the java. Smoking, physical activity, weight, tea drinking, blood pressure and cholesterol were all taken into account in this research.
This research did not seem to be dose-dependent: those that drank one cup of coffee a day or four had the same percentage of fewer strokes. Even with these results, the mechanism of action is unknown. There have even been some studies showing that because of the high antioxidant amounts in coffee, it improves insulin sensitivity and glucose metabolism. Thus, it is beneficial for those with diabetes by improving the body's response to insulin! Why is drinking coffee associated with lower stroke risk, less hospitalizations due to arrhythmias and better insulin sensitivity? Is it truly a miracle drug after all?
The coffee and arrhythmia link: http://www.sciencenews.org/view/generic/id/56862/title/Coffee_not_linked_to_heart_arrhythmia
The coffee and stroke link: http://www.sciencenews.org/view/generic/id/56701/title/Coffee_associated_with_lower_stroke_risk
Friday, June 18, 2010
How and what do Potassium and Calcium Channel Blockers block?
Many patients may hear that the medication that their doctor is prescribing them is a sodium channel blocker, Beta-blocker, potassium channel blocker, or a calcium channel blocker without being told what the difference is or why or how they work so well. Patients may be wondering...is Beta the letter of my fraternity that has come back to haunt me after all these years? As shown in the previous blog and will be further represented in this blog, sodium, "Beta", potassium and calcium are not some evil little molecules out to get your heart. They are very vital aspects of your bodily functions but can sometimes become overstimulated, cause arrhythmias and those funky channel blockers become just what the doctor orders. In the previous blog, I reviewed Sodium and Beta channel blockers. Here I will discuss Potassium and Calcium Channel blockers.
Class III: Potassium Channel Blockers
Action Potentials and the Role Potassium Plays in Action Potentials
Remember the action potentials discussed with the sodium channels? The beginning of the action potential starts with the depolarization of the cell membrane when sodium rushes in. The cell begins to repolarize when potassium leaves the cell, although not as quickly as the sodium rushes in. This repolarization brings the cell membrane back down to a more negative resting potential.
What a Potassium Channel Blocker Blocks and What They are Used for Treating
Potassium Channel Blockers bind to and block the potassium channels that are responsible for the cell membrane repolarization. Blocking these channels slows (delays) repolarization, which leads to an increase in action potential duration and an increase in the effective refractory period. An increase in the refractory period means the period of time that the cell is unexcitable and therefore cannot receive another action potential is prolonged. On an electrocardiogram, this delay of the depolarization increases the QT interval.
By making the cell less excitable, Potassium Channel Blockers are very effective in treating tachycardias. They are also known to treat supraventricular and ventricular arrythmias, atrial fibrillation, and atrial flutter.
Examples of Potassium Channel Blockers and Their Side Effects
Amiodarone, Dronedarone, Bretylium, Ibutilide, Dofetilide
The side effects of Potassium Channel Blockers are to produce a type of ventricular tachycardia, bradycardia and atrioventricular block or SA node dysfunction. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class IV: Calcium Channel Blockers
What are Calcium Channels and Where are They Found
Calcium channels are cells known as "excitable cells" that are sensitive to electrical impulses. Like the sodium and potassium channels, when the proteins receive the correct signal, the channel opens, allowing calcium to flow across the channel. The small charge that the calcium ion carries can stimulate muscle contractions, hormone release or firing of a neurotransmitter. Therefore, calcium channels are found in muscles, glial cells and neurons.
What a Calcium Channel Blocker Blocks and What They are Used for Treating
Calcium Channel Blockers dilate the arteries in the heart, reducing blood pressure in the arteries which leads to the heart being able to pump blood more easily. Essentially the heart's need for oxygen to pump the heart is lowered because it does not need to pump as often.
Calcium channel blockers are often used for high blood pressure, chest pain (due to lack of oxygen in the heart), and arrhythmias such as atrial fibrillation, and supraventricular tachycardia. They can be used after a heart attack for a patient that is not a good candidate for beta-blockers. Unfortunately, calcium channel blockers have not been shown to prevent future heart attacks.
Examples of Calcium Channel Blockers and Their Side Effects
Amlodipine, Diltiazem (Brand=Cardizem), Felodipine, Nifedipine, Nicardipine, Nimodipine, Nisoldipine, Verapamil
The most common side effects of Calcium Channel Blockers are constipation, nausea, headache, rash, swelling, low blood pressure, drowsiness and dizziness. In addition, liver dysfunction, sexual dysfunction and overgrowth of gums may occur. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class III: Potassium Channel Blockers
Action Potentials and the Role Potassium Plays in Action Potentials
Remember the action potentials discussed with the sodium channels? The beginning of the action potential starts with the depolarization of the cell membrane when sodium rushes in. The cell begins to repolarize when potassium leaves the cell, although not as quickly as the sodium rushes in. This repolarization brings the cell membrane back down to a more negative resting potential.
What a Potassium Channel Blocker Blocks and What They are Used for Treating
Potassium Channel Blockers bind to and block the potassium channels that are responsible for the cell membrane repolarization. Blocking these channels slows (delays) repolarization, which leads to an increase in action potential duration and an increase in the effective refractory period. An increase in the refractory period means the period of time that the cell is unexcitable and therefore cannot receive another action potential is prolonged. On an electrocardiogram, this delay of the depolarization increases the QT interval.
By making the cell less excitable, Potassium Channel Blockers are very effective in treating tachycardias. They are also known to treat supraventricular and ventricular arrythmias, atrial fibrillation, and atrial flutter.
Examples of Potassium Channel Blockers and Their Side Effects
Amiodarone, Dronedarone, Bretylium, Ibutilide, Dofetilide
The side effects of Potassium Channel Blockers are to produce a type of ventricular tachycardia, bradycardia and atrioventricular block or SA node dysfunction. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class IV: Calcium Channel Blockers
What are Calcium Channels and Where are They Found
Calcium channels are cells known as "excitable cells" that are sensitive to electrical impulses. Like the sodium and potassium channels, when the proteins receive the correct signal, the channel opens, allowing calcium to flow across the channel. The small charge that the calcium ion carries can stimulate muscle contractions, hormone release or firing of a neurotransmitter. Therefore, calcium channels are found in muscles, glial cells and neurons.
What a Calcium Channel Blocker Blocks and What They are Used for Treating
Calcium Channel Blockers dilate the arteries in the heart, reducing blood pressure in the arteries which leads to the heart being able to pump blood more easily. Essentially the heart's need for oxygen to pump the heart is lowered because it does not need to pump as often.
Calcium channel blockers are often used for high blood pressure, chest pain (due to lack of oxygen in the heart), and arrhythmias such as atrial fibrillation, and supraventricular tachycardia. They can be used after a heart attack for a patient that is not a good candidate for beta-blockers. Unfortunately, calcium channel blockers have not been shown to prevent future heart attacks.
Examples of Calcium Channel Blockers and Their Side Effects
Amlodipine, Diltiazem (Brand=Cardizem), Felodipine, Nifedipine, Nicardipine, Nimodipine, Nisoldipine, Verapamil
The most common side effects of Calcium Channel Blockers are constipation, nausea, headache, rash, swelling, low blood pressure, drowsiness and dizziness. In addition, liver dysfunction, sexual dysfunction and overgrowth of gums may occur. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Tuesday, June 15, 2010
How and what do all of these medication Blockers block?
Many patients may hear that the medication that their doctor is prescribing them is a sodium channel blocker, Beta-blocker, potassium channel blocker, or a calcium channel blocker without being told what the difference is or why or how they work so well. Patients may be wondering...is Beta the letter of my fraternity that has come back to haunt me after all these years? As you will see, sodium, "Beta", potassium and calcium are not some evil little molecules out to get your heart. They are very vital aspects of your bodily functions but can sometimes become overstimulated, cause arrhythmias and those funky channel blockers become just what the doctor orders. For now, I will just review Sodium Channel Blockers and Beta Blockers. Please stay tuned for a future blog in which I will review Potassiam and Calcium Channel-Blockers.
Class I: Sodium Channel Blockers
Action Potentials & The Role Sodium Channels Play in Action Potentials
An action potential is a short-lasting event in which the electrical membrane potential of a cell rapidly rises and falls. These occur in excitatory cells, such as neurons. In muscle cells, an action potential is the first step in the chain of events leading to contraction. Action potentials are often referred to as "spikes" or a neuron "firing." They are generated by special types of voltage-gated ion channels spanning the cell membrane. When the cell is resting, the channels are closed and are inactive. But if the membrane potential increases to a defined threshold value, the channels quickly open and allow ion movement across the membrane. This opening of the ion channels allows sodium to move into the cell, which further increases the membrane potential. More sodium channels open as a result, producing a greater electrical current. When all of the sodium ion channels are open, the cell is now more positive on the inside than on the outside; therefore, positive charge will want to leave the cell to attempt to reach the original threshold value at the resting potential. Therefore potassium channels are opened and potassium is released from the cell and the cell returns to its resting potential.
What a Sodium Channel Blocker Blocks and What They are Used for Treating
Sodium channel blockers reduce the exitogenicity of the cell membranes. Usually the phase depolarization (the moment that sodium usually flows in quickly and causes the cell to become more positive) is depressed. This prolongs the action potential by slowing conduction and decreases conductivity.
Sodium channel blockers are used for treating atrial fibrillation(Class Ia), atrial flutter (Ia), supraventricular (Ia) and ventricular tachyarrhythmias (Class Ia & IIb & Ic).
Examples of Sodium Channel Blockers and Their Side Effects
Ia: Quinidine, Procainamide, Disopryamide
Ib: Lidocaine, Tocainide, Mexiletine, Phenytoin (Brand=Dilantin)
Ic: Flecainide, Propafenone, Moricizine
Side effects include: Tachycardia, dry mouth, urinary retention, blurred vision, constipation, diarrhea, nausea, headache, and dizziness. Of course, not all Sodium Channel blockers have all of these side effects. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class II: Beta-Blockers
How Beta Receptors Normally Operate
Most people have experienced adrenaline rushes and know that it's a chemical that does some quite amazing things to our bodies. Adrenaline is also known as epinephrine and it acts by binding to receptors on the outside (membrane) of our cells. The receptors specialized for epinephrine are called Beta-adrenergic receptors and are made of 7 alpha helices spanning the cell membrane. Once epinephrine is bound to the receptor, the receptor is activated and a signal transduction cascade begins that ultimately stimulates the breakdown of glycogen for energy. First, the cytoplasmic loops (inside the cell) that connect the alpha helices together change their conformation. A β-adrenergic receptor mediates its effects via a class of peripheral membrane proteins known as the heterotrimeric G-proteins. It has 3 subunits, alpha (α), beta (β), and gamma (γ). In the inactive state, GDP is bound to the alpha subunit and when activated, this GDP molecule leaves and GTP takes its place. The beta-gamma dimer dissociates from the alpha subunit. This activation of the G protein activates adenylyl cyclase, which activates cyclic AMP (cAMP). cAMP bind to Protein Kinase A (PKA), activating PKA. PKA is a key regulator of the breakdown of glycogen and the body receives a sudden burst of energy!
What a Beta-Blocker Blocks and What They are Used for Treating
Beta-blockers are drugs that block norepinephrine and epinephrine (adrenaline) from binding to beta receptors on nerves. By blocking these neurotransmitters' effects, beta blockers reduce heart rate, reduce blood pressure by dilating blood vessels and may constrict air passages by stimulating the muscles that surround the air passages to contract. There are three types of beta receptor that control a variety of functions based on their location in the body. Beta-1 receptors are located in the heart, eye and kidneys; Beta-2 receptors are located in the lungs, GI tract, liver, uterus, blood vessels and skeletal muscle; Beta-3 receptors are located in fat cells. Beta blockers primarily block the Beta-1 and Beta-2 receptors.
Beta blockers are used for treating arrhythmia (irregular heart rhythms), high blood pressure, heart failure, chest pain (angina), tremors and sometimes prevention of migraines. They are also used after heart attacks to prevent further heart attacks.
Examples of Beta-blockers and Their Side Effects
As you will notice, the Beta-blockers listed below all end in "-lol."
Acebutolol
Atenolol
Bisoprolol
Carvedilol (Coreg)
Metoprolol (Toprol or Lopressor)
Nadolol
Pindolol
Propranolol
Sotalol
Timolol
The side effects of beta blockers may cause diarrhea, stomach cramps, nausea, vomiting, rash, blurred vision, muscle cramps, fatigue, headache, dizziness, confusion, depression, nightmares, hallucinations, shortness of breath in asthmatics and may cause low blood pressure. Of course, not all Beta-blockers have all of these side effects. Sudden withdrawal of Beta blockers may worsen chest pain and cause heart attacks. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class I: Sodium Channel Blockers
Action Potentials & The Role Sodium Channels Play in Action Potentials
An action potential is a short-lasting event in which the electrical membrane potential of a cell rapidly rises and falls. These occur in excitatory cells, such as neurons. In muscle cells, an action potential is the first step in the chain of events leading to contraction. Action potentials are often referred to as "spikes" or a neuron "firing." They are generated by special types of voltage-gated ion channels spanning the cell membrane. When the cell is resting, the channels are closed and are inactive. But if the membrane potential increases to a defined threshold value, the channels quickly open and allow ion movement across the membrane. This opening of the ion channels allows sodium to move into the cell, which further increases the membrane potential. More sodium channels open as a result, producing a greater electrical current. When all of the sodium ion channels are open, the cell is now more positive on the inside than on the outside; therefore, positive charge will want to leave the cell to attempt to reach the original threshold value at the resting potential. Therefore potassium channels are opened and potassium is released from the cell and the cell returns to its resting potential.
What a Sodium Channel Blocker Blocks and What They are Used for Treating
Sodium channel blockers reduce the exitogenicity of the cell membranes. Usually the phase depolarization (the moment that sodium usually flows in quickly and causes the cell to become more positive) is depressed. This prolongs the action potential by slowing conduction and decreases conductivity.
Sodium channel blockers are used for treating atrial fibrillation(Class Ia), atrial flutter (Ia), supraventricular (Ia) and ventricular tachyarrhythmias (Class Ia & IIb & Ic).
Examples of Sodium Channel Blockers and Their Side Effects
Ia: Quinidine, Procainamide, Disopryamide
Ib: Lidocaine, Tocainide, Mexiletine, Phenytoin (Brand=Dilantin)
Ic: Flecainide, Propafenone, Moricizine
Side effects include: Tachycardia, dry mouth, urinary retention, blurred vision, constipation, diarrhea, nausea, headache, and dizziness. Of course, not all Sodium Channel blockers have all of these side effects. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Class II: Beta-Blockers
How Beta Receptors Normally Operate
Most people have experienced adrenaline rushes and know that it's a chemical that does some quite amazing things to our bodies. Adrenaline is also known as epinephrine and it acts by binding to receptors on the outside (membrane) of our cells. The receptors specialized for epinephrine are called Beta-adrenergic receptors and are made of 7 alpha helices spanning the cell membrane. Once epinephrine is bound to the receptor, the receptor is activated and a signal transduction cascade begins that ultimately stimulates the breakdown of glycogen for energy. First, the cytoplasmic loops (inside the cell) that connect the alpha helices together change their conformation. A β-adrenergic receptor mediates its effects via a class of peripheral membrane proteins known as the heterotrimeric G-proteins. It has 3 subunits, alpha (α), beta (β), and gamma (γ). In the inactive state, GDP is bound to the alpha subunit and when activated, this GDP molecule leaves and GTP takes its place. The beta-gamma dimer dissociates from the alpha subunit. This activation of the G protein activates adenylyl cyclase, which activates cyclic AMP (cAMP). cAMP bind to Protein Kinase A (PKA), activating PKA. PKA is a key regulator of the breakdown of glycogen and the body receives a sudden burst of energy!
What a Beta-Blocker Blocks and What They are Used for Treating
Beta-blockers are drugs that block norepinephrine and epinephrine (adrenaline) from binding to beta receptors on nerves. By blocking these neurotransmitters' effects, beta blockers reduce heart rate, reduce blood pressure by dilating blood vessels and may constrict air passages by stimulating the muscles that surround the air passages to contract. There are three types of beta receptor that control a variety of functions based on their location in the body. Beta-1 receptors are located in the heart, eye and kidneys; Beta-2 receptors are located in the lungs, GI tract, liver, uterus, blood vessels and skeletal muscle; Beta-3 receptors are located in fat cells. Beta blockers primarily block the Beta-1 and Beta-2 receptors.
Beta blockers are used for treating arrhythmia (irregular heart rhythms), high blood pressure, heart failure, chest pain (angina), tremors and sometimes prevention of migraines. They are also used after heart attacks to prevent further heart attacks.
Examples of Beta-blockers and Their Side Effects
As you will notice, the Beta-blockers listed below all end in "-lol."
Acebutolol
Atenolol
Bisoprolol
Carvedilol (Coreg)
Metoprolol (Toprol or Lopressor)
Nadolol
Pindolol
Propranolol
Sotalol
Timolol
The side effects of beta blockers may cause diarrhea, stomach cramps, nausea, vomiting, rash, blurred vision, muscle cramps, fatigue, headache, dizziness, confusion, depression, nightmares, hallucinations, shortness of breath in asthmatics and may cause low blood pressure. Of course, not all Beta-blockers have all of these side effects. Sudden withdrawal of Beta blockers may worsen chest pain and cause heart attacks. Talk with your doctor and your pharmacist to find out what the right drug is for you. And don't forget to rate the drug on www.RateaDrug.com to let others know what experiences you had with a specific medication!
Friday, June 11, 2010
Existing Pharmacological Treatments for Arrhythmia
Pharmacological treatment includes administering antiarrhythmic medications like the ones listed on this page in addition to hundreds of others. A complete list of antiarrhyhmic medications can be seen on http://rateadrug.com/Arrhythmia-Irregular-Heartbeat-symptoms-feedback.aspx . Normally because antiarrhythmic agents have a narrow toxic-therapeutic relationship, important compications of therapy can results from amounts of drug that only slightly exceed the amount necessary to produce beneficial effects. It is obvious that careful dosage is essential to maintain adequate but nontoxic amounts of drug in the body. There are many factors to consider when prescribing an antirarrhythmic medication: tissue type, the degree of acute or chronic damage, heart rate, membrane potential, heart rate, intrinsic tissue properties, orientation of myocardial fibers and other associated conditions. It therefore may take multiple attempts for a doctor to find the medication that is right for the patient. Tachycardias (beating too fast) and premature beats may be administered intravenously in an emergency situation or orally for long term treatment. Antiarrhythmic drugs can either suppress the quick-firing pacemaker tissue or depress the transmission of impulses that conduct too rapidly. In patients with atril fibrillation, a blood thinner is usually added to reduce the risk of blood clots and stroke. The effectiveness of antiarrhythmic drugs can be gauged by an electrocardiogram.
Most of the available antiarrhythmic drugs are grouped into four main classes according to Vaughan Williams classification: (I) Sodium Channel Blockers, (II) Beta-Blockers, (III) Potassium Channel Blockers and (IV) Calcium Channel Blockers. In most cases, the drugs have to be taken for the rest of the patient's life.
Class I: Sodium Channel Blockers
Sodium (Na) channel blockers slow conduction in fast-channel tissues by blocking fast sodium channels. These drugs are used for patients with ventricular arrhythmias or recurrent atrial fibrillation. These drugs are typically only used in patients who do not have a structural heart disorder because they may depress ventricular contractility. Some commonly prescribed sodium channel blockers are (generic, brand):
Disopyramide (Norpace)
Flecainide (Tambocor)
Lidocaine (Xylocaine)
Quinidine
Phenytoin (Dilantin)
Class II: Beta-Blockers
Beta-blockers decrease the heart rate and cardiac output, which lowers blood pressure by blocking the effects of adrenaline (what mediates the "fight or flight" response). They affect predominantly slow-channel tissues (SA and AV nodes), where they decrease rate of automaticity, slow conduction velocity and prolong refractoriness. These are used to treat sinus tachycardia, atrial flutter and atrial fibrillation. They are also used to treat chest pain. These are not to be used in patients with asthma. Some commonly prescribed beta-blockers are (generic, brand):
Acebutolol (Sectral)
Atenolol (Tenormin)
Metoprolol (Lopressor)
Nadolol (Corgard)
Propranolol (Inderal)
Class III: Potassium Channel Blockers
Potassium channel blockers prolong action potential duration and refractoriness in slow and fast channel tissues. The conduction velocity is not significantly affected but the capacity for the cardiac tissue to transmit impulses at high frequencies is reduced. These are helpful in patients with atrial flutter, atrial fibrillation and ventricular tachycardias. Some commonly prescribed potassium channel blockers are (generic, brand):
Amiodarone (Pacerone)
Dofetilide (Tikosyn)
Ibutilide (Corvert)
Sotalol (Betapace)
Class IV: Calcium Channel Blockers
Calcium channel blockers slow the heart rate by interrupting the movement of calcium into the heart. These are used to treat high blood pressure, chest pain and arrhythmias. These depress calcium dependent action potentials in slow channel tissues and thus decrease the rate of automaticity, slow conduction velocity and prolong refractoriness. These are especially helpful for patients with atrial fibrillation and supraventricular tachycardia. Some commonly prescribed calcium channel blockers (generic, brand):
Amlodipine (Norvasc)
Diltiazem (Cardizem)
Felodipine (Plendil)
Nifedipine (Procardia)
Verapamil (Covera)
As mentioned above, you can visit www.RateADrug.com to learn about others' experiences with most of the medications listed above. If you would like to let others know about your experience with a particular drug, fill out an anonymous 5 minute survey by clicking on Evaluate This Treatment! I hope you can find something to assist you in your journey with arrhythmia. If you have any questions or comments, please let me know!
Most of the available antiarrhythmic drugs are grouped into four main classes according to Vaughan Williams classification: (I) Sodium Channel Blockers, (II) Beta-Blockers, (III) Potassium Channel Blockers and (IV) Calcium Channel Blockers. In most cases, the drugs have to be taken for the rest of the patient's life.
Class I: Sodium Channel Blockers
Sodium (Na) channel blockers slow conduction in fast-channel tissues by blocking fast sodium channels. These drugs are used for patients with ventricular arrhythmias or recurrent atrial fibrillation. These drugs are typically only used in patients who do not have a structural heart disorder because they may depress ventricular contractility. Some commonly prescribed sodium channel blockers are (generic, brand):
Disopyramide (Norpace)
Flecainide (Tambocor)
Lidocaine (Xylocaine)
Quinidine
Phenytoin (Dilantin)
Class II: Beta-Blockers
Beta-blockers decrease the heart rate and cardiac output, which lowers blood pressure by blocking the effects of adrenaline (what mediates the "fight or flight" response). They affect predominantly slow-channel tissues (SA and AV nodes), where they decrease rate of automaticity, slow conduction velocity and prolong refractoriness. These are used to treat sinus tachycardia, atrial flutter and atrial fibrillation. They are also used to treat chest pain. These are not to be used in patients with asthma. Some commonly prescribed beta-blockers are (generic, brand):
Acebutolol (Sectral)
Atenolol (Tenormin)
Metoprolol (Lopressor)
Nadolol (Corgard)
Propranolol (Inderal)
Class III: Potassium Channel Blockers
Potassium channel blockers prolong action potential duration and refractoriness in slow and fast channel tissues. The conduction velocity is not significantly affected but the capacity for the cardiac tissue to transmit impulses at high frequencies is reduced. These are helpful in patients with atrial flutter, atrial fibrillation and ventricular tachycardias. Some commonly prescribed potassium channel blockers are (generic, brand):
Amiodarone (Pacerone)
Dofetilide (Tikosyn)
Ibutilide (Corvert)
Sotalol (Betapace)
Class IV: Calcium Channel Blockers
Calcium channel blockers slow the heart rate by interrupting the movement of calcium into the heart. These are used to treat high blood pressure, chest pain and arrhythmias. These depress calcium dependent action potentials in slow channel tissues and thus decrease the rate of automaticity, slow conduction velocity and prolong refractoriness. These are especially helpful for patients with atrial fibrillation and supraventricular tachycardia. Some commonly prescribed calcium channel blockers (generic, brand):
Amlodipine (Norvasc)
Diltiazem (Cardizem)
Felodipine (Plendil)
Nifedipine (Procardia)
Verapamil (Covera)
As mentioned above, you can visit www.RateADrug.com to learn about others' experiences with most of the medications listed above. If you would like to let others know about your experience with a particular drug, fill out an anonymous 5 minute survey by clicking on Evaluate This Treatment! I hope you can find something to assist you in your journey with arrhythmia. If you have any questions or comments, please let me know!
Wednesday, June 9, 2010
Existing Nonpharmacological Treatments for Arrhythmia
Conventional treatment modalities include surgery, insertion of medical devices, nonsurgical interventions and pharmacological treatment including medications. Surgical interventions include open-heart maze procedure, ventricular aneurysm surgery and coronary bypass surgery. Medical devices include placement of pacemakers and internal cardioverter defibrillator also known as an ICD. Nonsurgical intervention includes catheter radiofrequency ablation, cardioversion sometimes accompanied with drugs and electrical cardioversion. Pharmacological treatment includes administering antiarrhthymic medications, some of which are listed on this website and will be further discussed in a future post.
Surgery is often only recommended when other options listed above have failed. There are several surgery options available depending on the type of arrhythmia and other complicating factors. The maze procedure is used to treat atril fibrillation. The surgeon directs the heart's electrical activity in the proper order once the cuts have healed. It is called the maze procedure because the electrical impulse can only choose one correct "maze" to travel through. The second surgery, ventricular aneurysm surgery that removes the thinning of the ventricular wall that can be damaged after a heart attack. After a heart attack, the ventricle can become thin, weak and incapable of fully pumping. The third surgical option is a coronary bypass surgery and is usually used for those with serious coronary artery disease. The surgery involves rerouting the blood flow around the clogged artery.
Medical devices such as a pacemaker and ICDs are very common treatments for patients with an irregular heartbeat. For those with bradycardia (slow heartbeat), implantable pacemakers controls the heart's electrical stimulus when the heart's natural pacemaker (sinoatrial node) does not work as it should. The pacemaker can sense that the heart is not beating at the proper time and sends an electrical impulse to make the heart beat. The actual device of the pacemaker consists of a battery to provide power, leads to send the impulse and an electrode to sense each beat of the heart and delivers the electrical impulse when necessary. There are different types of pacemakers dependent on the heart rhythm and therefore vary in the number of leads they contain (one, two or three) and where they are placed (upper or lower chamber). The implantation procedure includes using local anesthesia and receive an additional IV medication for the patient to relax. An ICD or implantable cardioverter defibrillator is a device that acts as a pacemaker for slow heat rate but can also treat fast rhythms. It treats a fast rhythm by delivering the appropriate electrical therapy necessary, whether it be rapid-pacing, low-energy or high-energy shock. Most implantations are done using local anesthesia and possibly a sedative.
The nonsurgical options for treating arrhythmias include radio-frequency ablation and cardioversion. During the radio-frequency ablation, a catheter is placed next to the abnormal pathway and destroys the abnormal tissue. The catheter is inserted into a vein or artery and is commonly used for atrial flutter, supraventricular tachycardias, ventricular tachycardias and atrial fibrillation. The abnormal tissue is destroyed via heat ablation; once the tissue is eliminated, the rapid heart rhythm will be blocked and the rhythm should not occur. This procedure is done under sedation and uses local anesthesia, and may take anywhere from three to seven hours but the recovery time is short. Patients normally return to usual activities within seven days of the procedure. The second option for nonsurgical procedure to treat arrhythmia (particularly atrial flutter and atrial fibrillation) is cardioversion. During this procedure, the patient will be sedated, electrode patches will be placed on the patient's back and chest which are attached to a heart monitor. An electrical impulse will be delivered to the patient's heart through the two large patches to help it return to a normal rhythm. If necessary, multiple impulses will be given to return the heart to a normal rhythm. After the procedure, the patient will only remain in the hospital for a few hours. The only discomfort comes from skin burns on the chest and back where the patches were placed.
As mentioned above, these are just a few of the existing nonpharmacological treatments for irregular heartbeats. Any comments, questions or suggestions are welcome! Coming soon will be the existing pharmacological treatments!! Don't forget to check out www.rateadrug.com to rate drugs that have positively or negatively affected your journey with arrhythmia.
~Alicia
Surgery is often only recommended when other options listed above have failed. There are several surgery options available depending on the type of arrhythmia and other complicating factors. The maze procedure is used to treat atril fibrillation. The surgeon directs the heart's electrical activity in the proper order once the cuts have healed. It is called the maze procedure because the electrical impulse can only choose one correct "maze" to travel through. The second surgery, ventricular aneurysm surgery that removes the thinning of the ventricular wall that can be damaged after a heart attack. After a heart attack, the ventricle can become thin, weak and incapable of fully pumping. The third surgical option is a coronary bypass surgery and is usually used for those with serious coronary artery disease. The surgery involves rerouting the blood flow around the clogged artery.
Medical devices such as a pacemaker and ICDs are very common treatments for patients with an irregular heartbeat. For those with bradycardia (slow heartbeat), implantable pacemakers controls the heart's electrical stimulus when the heart's natural pacemaker (sinoatrial node) does not work as it should. The pacemaker can sense that the heart is not beating at the proper time and sends an electrical impulse to make the heart beat. The actual device of the pacemaker consists of a battery to provide power, leads to send the impulse and an electrode to sense each beat of the heart and delivers the electrical impulse when necessary. There are different types of pacemakers dependent on the heart rhythm and therefore vary in the number of leads they contain (one, two or three) and where they are placed (upper or lower chamber). The implantation procedure includes using local anesthesia and receive an additional IV medication for the patient to relax. An ICD or implantable cardioverter defibrillator is a device that acts as a pacemaker for slow heat rate but can also treat fast rhythms. It treats a fast rhythm by delivering the appropriate electrical therapy necessary, whether it be rapid-pacing, low-energy or high-energy shock. Most implantations are done using local anesthesia and possibly a sedative.
The nonsurgical options for treating arrhythmias include radio-frequency ablation and cardioversion. During the radio-frequency ablation, a catheter is placed next to the abnormal pathway and destroys the abnormal tissue. The catheter is inserted into a vein or artery and is commonly used for atrial flutter, supraventricular tachycardias, ventricular tachycardias and atrial fibrillation. The abnormal tissue is destroyed via heat ablation; once the tissue is eliminated, the rapid heart rhythm will be blocked and the rhythm should not occur. This procedure is done under sedation and uses local anesthesia, and may take anywhere from three to seven hours but the recovery time is short. Patients normally return to usual activities within seven days of the procedure. The second option for nonsurgical procedure to treat arrhythmia (particularly atrial flutter and atrial fibrillation) is cardioversion. During this procedure, the patient will be sedated, electrode patches will be placed on the patient's back and chest which are attached to a heart monitor. An electrical impulse will be delivered to the patient's heart through the two large patches to help it return to a normal rhythm. If necessary, multiple impulses will be given to return the heart to a normal rhythm. After the procedure, the patient will only remain in the hospital for a few hours. The only discomfort comes from skin burns on the chest and back where the patches were placed.
As mentioned above, these are just a few of the existing nonpharmacological treatments for irregular heartbeats. Any comments, questions or suggestions are welcome! Coming soon will be the existing pharmacological treatments!! Don't forget to check out www.rateadrug.com to rate drugs that have positively or negatively affected your journey with arrhythmia.
~Alicia
Subscribe to:
Comments (Atom)
